

Research Article | DOI: https://doi.org/10.31579/2834-5177/045
Identifying Dimensions and Components of Organizational Readiness for Knowledge Translation Implementation in Type I Medical Sciences Universities in Iran: A Scoping Review
- Hamed Hosseinzadeh 1
- Ali Sadatmoosavi 2*
- Oranus Tajedini 3
- Asghar Tavan 4
- Mohammad Azami 5
- Mousa YaminFiroo 6
1Candidate, Medical Library and Information Science, Faculty of Management and Medical Information Sciences, Kerman University of Medical Sciences,Kerman, Iran.
2Associate Professor , Department of Medical Library & Information Sciences, Faculty of Management and Medical Information Sciences, Kerman University of Medical Sciences., Kerman, Iran.
3Associate Professor, Department of Knowledge and Information Science, Shahid Bahonar University of Kerman, Kerman, Iran.
4Assistant professor, Health in Disasters and Emergencies Research Center, Institute for Futures Studies in Health, Kerman University of Medical Sciences, Kerman, Iran.
5Associate Professor, Department of Medical Library & Information Sciences, Faculty of Management and Medical Information Sciences, Kerman University of Medical Sciences., Kerman, Iran.
*Corresponding Author: Ali Sadatmoosavi, Department of Medical Library & Information Sciences, Faculty of Management and Medical Information Sciences, Kerman University of Medical Sciences., Kerman, Iran.
Citation: Hamed Hosseinzadeh, Ali Sadatmoosavi, Oranus Tajedini, Asghar Tavan, Mohammad Azami, et al, (2025), Identifying Dimensions and Components of Organizational Readiness for Knowledge Translation Implementation in Type I Medical Sciences Universities in Iran: A Scoping Review, International Journal of Clinical Infectious Diseases, 4(6); DOI:10.31579/2834-5177/045
Copyright: © 2025, Ali Sadatmoosavi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 November 2025 | Accepted: 18 November 2025 | Published: 28 November 2025
Keywords: organizational readiness; knowledge translation; medical universities
Abstract
Abstract
Introduction: Healthcare organizations must have the ability to adapt to rapid environmental changes and respond to evidence-based needs. One of the key prerequisites for the effective implementation of these changes is organizational readiness for knowledge translation (KT). The aim of this study is to identify the dimensions and components of organizational readiness for implementing KT in medical universities in Iran.
Methods: This research was conducted using a scoping review approach based on the Arksey and O'Malley framework. A comprehensive search was performed without a time limitation in international databases such as PubMed, Scopus, Web of Science, and Persian databases MagIran and SID. Out of 4540 identified documents, 14 articles were included after screening and final assessment.
Results: After extracting the dimensions and components from the reviewed studies, five dimensions and 14 components were identified, as follows: Organizational Climate (culture of readiness and innovation, intra- and inter-organizational interactions, organizational dynamics), Organizational Support (development and training opportunities, financial resources, capacity building and organizational performance improvement), Change Management (strategies and change implementation capacity, leadership support), Organizational Context (knowledge management in the organization, organizational structure and technological advancement, social capital), and Human Resources (self-efficacy and motivation, leadership, collaboration and participation).
Conclusion: To enhance organizational readiness for KT implementation, it is essential for health system managers and policymakers to understand the importance of utilizing research evidence and, through skill development and active participation in research processes, create the necessary environment for utilizing generated knowledge.
Introduction
Healthcare organizations are complex and highly adaptable entities operating in a dynamic environment. Policymakers and healthcare managers must utilize available credible research evidence for planning, organizing, leading, and controlling healthcare organizations (1). Knowledge translation, policy-making, and management of healthcare organizations lead to optimal use of scarce resources and increased efficiency (2). Given the evidence that successful KT activities can significantly impact health outcomes, it is crucial to create evidence and strategies that support such activities in low- and middle-income countries (3). Such approaches can also facilitate knowledge exchange and influence evidence-based information uptake by transforming institutions in low- and middle-income countries into knowledge brokers (specialized experts who bridge the gap between research and end-users) (4). Factors related to capacity, interest, ability, and skills of both producers and users of knowledge and the organizational environment of healthcare systems affect the knowledge process (1).
Management experts argue that organizational readiness for change is a critical prerequisite for the successful implementation and coping with change. Many organizational innovations fail due to the lack of organizational readiness (5). Organizational readiness assessment is a method that evaluates various dimensions of an organization, such as managerial and organizational aspects, human resources, structural, process, technical, infrastructural, and cultural aspects, to assess the readiness of each part of the organization for adopting management systems. In fact, readiness is a necessary prerequisite for an individual or an organization to successfully confront organizational change (6). Research on organizational readiness for KT can inform capacity-building strategies that enhance the uptake and successful implementation of KT activities. This can improve the national credibility of the institution, increase future KT opportunities, and open doors for new partnerships and financial resources. This motivation for institutional change ultimately facilitates achieving the overarching goal of reducing disease burden and mortality, which is one of the key objectives of KT activities (3).
One of the concerns in the global healthcare system is the lack of credible evidence and research-derived knowledge (7). Despite the exponential growth in publications related to the importance of KT across different health sciences, there is still a significant gap between what is being done (practice) and what is known (evidence) at all levels of healthcare decision-making (8). In Iran, despite significant growth in domestic research in the health system field in recent years, research is still in its infancy. As a result, policymakers often face a lack of reliable evidence when addressing many questions (9). Since one of the challenges of the health system is the need for research to support policy-making, it is necessary to develop applied research in the health system, especially in the field of KT (10). Considering these issues and their importance, this research aims to identify the dimensions and components of organizational readiness for implementing KT in medical universities in Iran.
Materials and Methods:
This study was conducted using a scoping review approach based on the five-stage framework proposed by Arksey and O'Malley (2005). The stages include: 1) Formulation of the research question, 2) Identification of relevant studies, 3) Selection of eligible studies, 4) Extraction and categorization of data, and 5) Analysis, synthesis, and presentation of results [11]. This approach was chosen to comprehensively and systematically explore key concepts in the studied area, particularly in emerging and complex topics such as organizational readiness for KT implementation.
Scoping reviews enable the integration and analysis of a wide range of published and unpublished studies, providing a broad view of the various dimensions of a phenomenon, especially when the goal is to go beyond measuring the effectiveness of an intervention and focus on elucidating frameworks and conceptual models [12].
Stage 1:
Formulation of the Research Question
The main research question was: "What are the dimensions and components of organizational readiness in Iranian medical universities for the effective implementation of knowledge translation?"
Stage 2:
Identification of Relevant Studies
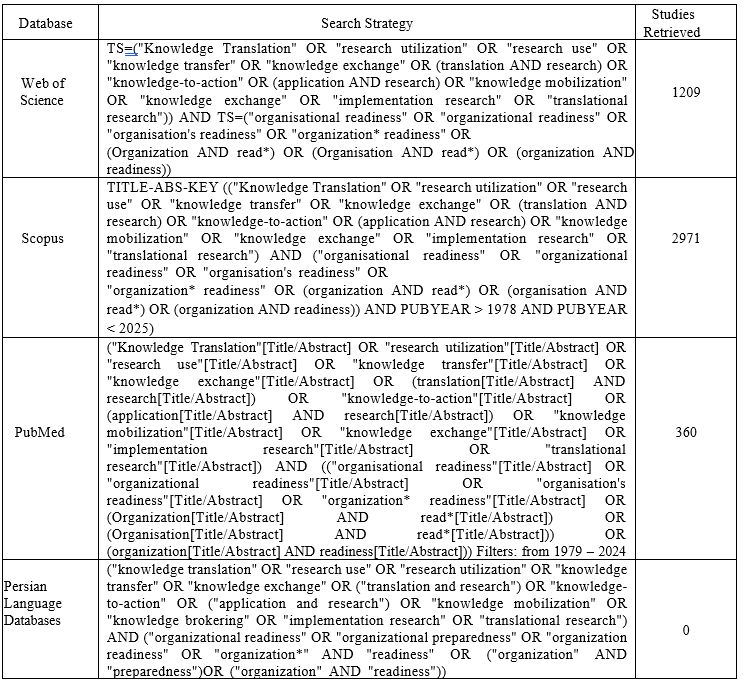
No time limitations were set for the search. Electronic searches were conducted in credible international databases, including PubMed, Scopus, Web of Science, and Google Scholar. For Persian articles, MagIran and SID databases were reviewed. The key search terms included: Translation of knowledge, use of research, knowledge transfer, knowledge exchange, knowledge into practice, knowledge mobilization, organizational readiness, organization and reading, organization and readiness In Persian-language databases, equivalent MeSH terms in Farsi were used accordingly (see Table 1).
Inclusion criteria were: 1) Articles in Persian and English, and 2) Studies related to organizational readiness and KT in health. Exclusion criteria were: 1) Irrelevant articles, and
2) Articles published in languages other than Persian and English
Stage 3:
Selection of Eligible Studies
A total of 4540 articles were retrieved from the mentioned databases. Data were managed using EndNote software, and after removing duplicates (n=1674), 2866 articles were left for title and abstract screening. Subsequently, 2819 articles were excluded due to content mismatch, and 47 articles were selected for full-text review. Finally, 14 articles were included in the analysis (The PRISMA-ScR flowchart is presented in Figure 1).
Stage 4:
Extraction and Categorization of Data
The key data from the selected studies were summarized and categorized in Table 2. These data included study objectives, methodologies, tools used, and the dimensions and components identified regarding organizational readiness for KT.
Stage 5:
Analysis and Presentation of Results
Based on content analysis of the selected studies, five main dimensions and fourteen components were identified and extracted as a conceptual framework for organizational readiness to implement KT in Iranian medical universities (Figure 1).
Results:
Analysis of the results from the search indicated that the majority of the retrieved articles came from the Scopus database (2971 articles), followed by PubMed (360 articles) and Web of Science (1209 articles). However, in Persian-language databases like MagIran and SID, due to the novelty of the topic and limited relevant studies, no articles met the inclusion criteria (Flowchart).
It is noteworthy that a significant portion of the retrieved articles were focused on two separate domains: "Organizational Readiness" and "Knowledge Translation," with only a few addressing the relationship between the two. After final screening, 14 relevant articles were selected for final analysis.
Discussion and Conclusion:
The findings of this scoping review study revealed that organizational readiness for implementing knowledge translation in medical universities in Iran consists of five key dimensions: organizational climate, organizational support, change management, organizational context, and human resources, which can be analyzed through 14 subcomponents. These dimensions and components are directly related to the organization's ability to plan, make decisions, and effectively execute knowledge translation activities.
Organizational climate has been identified as one of the key dimensions of organizational readiness for implementing knowledge translation in 7 out of the 14 reviewed studies. This dimension refers to the organizational environment and culture, which can either support or hinder knowledge translation activities [13]. According to the findings of the reviewed studies, the components of this dimension include readiness culture, readiness for innovation, intra- and inter-organizational interactions, and organizational dynamics.
The study by Kalbarczyk et al. (2024) showed that, in the context of knowledge translation readiness, organizational climate (at the organizational level) is more relevant for younger individuals, while self-efficacy (at the individual level) is more significant for middle-aged and older groups [13]. This finding suggests that less experienced individuals may rely more on internal support for knowledge translation, as they do not yet have sufficient external networks and resources. In contrast, more experienced individuals, with greater mastery, feel more control over their environment and have greater confidence in their ability to implement knowledge translation.
Other studies have also emphasized the importance of organizational climate in supporting organizational dynamics. For example, the findings of Grandes et al. (2017) and Attieh et al. (2014) suggest that a favorable organizational climate facilitates positive organizational changes, strengthens trust among employees, and promotes collaboration between them [14,15].
The results of several other studies also confirm the impact of organizational climate on the knowledge-sharing process within organizations. Among these studies are those by Akram et al. (2020) [16], Fatemi et al. (2022) [17], Kaffashan Kakhki et al. (2020) [18], Mbandi (2020) [19], Usmanova et al. (2020) [20], and Vandavasi et al. (2020) [21]. The findings of these studies indicate that organizational climate can either facilitate or hinder knowledge interactions among employees.
For instance, the study by Kuo et al. (2014) showed that a supportive organizational climate increases employees' intrinsic motivation to share and receive knowledge, while a negative perception of organizational culture prevents knowledge exchange among colleagues [22]. Additionally, Betes and Khasawneh (2005) confirmed that organizational climate influences employees' perceptions of the prevailing culture [23]. The findings of Banerjee et al. (2017) also showed that a positive organizational climate can facilitate knowledge sharing among employees [24]. Overall, organizational climate can be seen as a soft yet effective foundation for the success of knowledge translation. Medical organizations should strengthen their organizational readiness by creating an innovation culture, fostering constructive interactions between units, and enhancing organizational dynamics to ensure the effective implementation of knowledge translation.
In the present review, organizational support was identified as one of the key dimensions of readiness for implementing knowledge translation in 7 out of the 14 reviewed studies. This dimension includes three main components: development and training opportunities, financial resources, and capacity building and performance improvement. Organizational support plays a fundamental role in creating the necessary infrastructure and providing the conditions required for the establishment and sustainability of knowledge translation in medical organizations. The study by Attieh et al. (2014) showed that this dimension is achieved through processes such as feedback, evaluation, monitoring, and creating a supportive climate. Moreover, the successful implementation of any organizational change requires an internal environment that can stabilize and institutionalize that change [15]. Our findings also emphasize that organizational support encompasses a range of requirements, including access to financial resources, supportive policies and procedures, training opportunities, and institutional and individual readiness. According to the study by Kalbarczyk et al. (2024), financial resources played a lesser role in the perception of readiness for knowledge translation among individuals in coordination roles. This finding may be due to the lesser involvement of these individuals in budgeting processes and financial resource management [13]. On the other hand, the study by Attieh et al. (2014) introduced the concept of "institutional readiness," which consists of motivation, values, organizational goals, and managerial and structural support [15]. In this context, systematic readiness assessment can help identify gaps and design targeted strategies for enhancing knowledge translation. Studies conducted in Iran have also confirmed the importance of this dimension. Specifically, the research by Shams and Abbasi-Kasani (2017), Ghanbari et al. (2017), Lotfi et al. (2016), Diba Vajari et al. (2016), and Youzbashi et al. (2016) showed that managerial support was the most important facilitating factor in the successful transfer of education and the implementation of knowledge programs in healthcare organizations. These findings align with the results of studies by Kontoghiorghes (2014), Lancaster (2016), and Park et al. (2018), which highlighted the role of structural and managerial support in the success of knowledge translation [25-32]. Overall, the dimension of organizational support, by providing resources, structures, learning opportunities, and capacity building, forms the essential infrastructure required for the readiness and successful implementation of knowledge translation.
In this scoping review, change management was identified in 7 out of the 14 reviewed studies as one of the key dimensions of organizational readiness for implementing knowledge translation (KT). This dimension refers to the organization’s ability to plan, lead, execute, and institutionalize changes required for the successful implementation of KT activities. Accordingly, organizational members share beliefs about their collective ability to manage and implement change [13]. Findings from this review indicate that change management includes two main components: capacity to implement organizational change, leadership support for change, and shifts in managerial strategies.
Kalbarczyk et al. (2021) emphasized that assessing organizational readiness can serve as an effective tool for identifying facilitators and barriers to implementing capacity-building strategies. This assessment can also enable organizations to tailor their approaches to overcome obstacles in implementing KT [3]. The study by Kalbarczyk et al. (2024) further highlighted the role of leadership and gender in the effectiveness of organizational change. Their findings indicate that active engagement of organizational leaders and promotion of women’s leadership can enhance the effectiveness of KT-related changes [13].
Strauss et al. (2009) reported that the effectiveness of change at the organizational level contributed more significantly to readiness for KT among men compared to women. Additionally, for individuals in leadership roles, the effectiveness of change was less significant than for those in other professional roles. Nevertheless, supportive leadership, while not sufficient on its own, is recognized as an important and well-documented component of the organizational change management process [25].
In line with this, the study by Shea et al. (2014) evaluated the psychometric properties of organizational readiness assessment tools, including the change effectiveness scale. In these tools, change effectiveness was primarily based on trust in the ability to manage the change process, coordination of tasks, and organizational investment motivation. The related items in the present study similarly describe elements of trust, motivation, and readiness for change [26].
From a theoretical standpoint, organizational members may commit to change for different reasons—some may perceive it as valuable, while others may feel obliged or responsible. It is reasonable to assume that the perspectives and actions of external stakeholders may also influence these values and commitments, particularly in health-related institutions [3]. The concept of the “change process” refers to the set of actions pursued to effectively implement organizational change. This process includes managerial support, external influences, and perceived options for change.
According to the model proposed by Armenakis and Harris (2002), this process consists of three stages: readiness, adoption, and institutionalization. Since these stages do not occur automatically, managers must design and implement intelligent, capacity-aligned programs to foster ongoing readiness for change among staff members [27]. Complementing this framework, Armenakis et al. (2011) defined readiness for change as a combination of beliefs, attitudes, and behavioral intentions that reflect both individual and organizational perceptions of the feasibility of successful change [28].
Therefore, the success of medical universities in implementing knowledge translation requires simultaneous attention to change strategies, the capacity to execute them, and supportive leadershipIn the present scoping review, the dimension of organizational context was identified in 7 out of the 14 final studies as one of the core components of organizational readiness for knowledge translation (KT). This dimension refers to the capacities, infrastructures, and contextual features of an organization that either facilitate or hinder the effective implementation of KT. Various levels of organizational context involve skill and training deficiencies among researchers and policymakers, weaknesses in institutional infrastructure, and insufficient human and technical resources [3].
Gagnon et al. (2019) demonstrated that assessing the organizational context—including resources, infrastructure, and external factors—can play a crucial role in the success or failure of KT processes [29]. Similarly, Kalbarczyk et al. (2021) emphasized that organizational structures such as physical spaces, specialized training, and adequate human resources are essential prerequisites for supporting KT activities [3]. According to our findings, the organizational context dimension includes four key components: knowledge management, organizational structure, technological advancement, and organizational social capital.
The study by Gagnon et al. (2011) showed the direct impact of organizational context on research utilization and highlighted the need for health systems to be adequately prepared to apply scientific evidence. Facilitating factors in this process include strong leadership, participatory decision-making, financial and institutional support, effective infrastructure, and dynamic organizational communication [30].
Kalbarczyk et al. (2021) also identified soft skills (e.g., communication, self-awareness, adaptability), robust professional networks, and alignment of organizational priorities and incentives as important drivers of KT capacity building in low- and middle-income countries (LMICs) [3]. In this regard, the capacity-building model proposed by Potter and Brough (2004) introduces interrelated and hierarchical dimensions including structures, systems, roles, staff, infrastructure, skills, and tools. According to this model, robust and systematic structures enable the optimal use of tools and skills to facilitate effective change [31].
El-Jardali and Fadlallah, in their KT framework, placed researcher capacity-building at the core and stressed that interventions should simultaneously target individual, team, institutional, and system levels [32]. Although institutional capacity is widely acknowledged as a prerequisite for the sustainable use of evidence, there is limited evidence on how to effectively implement capacity-building activities at this level [33].
In this framework, Attieh et al. (2014) categorized contextual organizational factors into two main subsets: appropriate human resources and sufficient material resources to support change, which were considered more critical than organizational culture [15]. Numerous other studies—including those by Weiner, Holt, and Kitson—have emphasized that without understanding and enhancing the organizational context, successful implementation of organizational changes, including KT, is unlikely [5, 34, 35]. These factors include adequate human and material resources, as well as an understanding of the prevailing organizational culture and climate in which change takes place [34, 36].
It is worth noting that capacity-building must align with the stage of organizational change, and strategies should be designed to facilitate the organization's growth and evolution according to the readiness level and needs at each phase of change [13]. Finally, Murunga et al. (2020) highlighted the need for further research into the facilitators and barriers affecting researchers' ability to successfully implement KT activities at both individual and organizational levels in LMICs [37].
In conclusion, it appears that medical science organizations must focus on the three main components of organizational context—knowledge management, structure and technology, and social capital—and simultaneously consider both internal and external factors to create the necessary conditions for effective KT implementation.
The human resources dimension was identified in 12 of the final included studies and is regarded as one of the most fundamental strategic assets of an organization. According to the findings of this review, the key components of this dimension include self-efficacy, leadership, motivation, interaction, and participation. Self-efficacy refers to individuals’ belief in their capability to contribute effectively to KT activities and plays a central role in personal readiness for engaging in organizational change processes (13, 41). The study by Kalbarczyk et al. (2021) also indicated that lack of training and necessary resources—such as time and personnel—constitutes a major challenge for KT implementation, and stressed the necessity of leadership engagement to strengthen KT efforts (3).Organizational leaders, through consistent messaging and action, can foster a shared vision for change among staff and help enhance motivation and engagement (38). Leadership traits that support change—such as high self-efficacy—are recognized as facilitators in creating an enabling environment for early-career researchers (39, 40). Furthermore, self-efficacy develops in interaction with the organizational context and grows through repeated mastery experiences and modeling (42). It is expected that more experienced staff, possessing higher levels of self-efficacy, will have greater confidence in their ability to implement KT.
Numerous studies have also confirmed the role of participatory leadership and fair treatment of employees in enhancing organizational trust, motivation, and effective engagement (43, 44). For instance, Buchan et al. (2005) found that involving staff in decision-making—even in the face of increased workload—leads to improved morale and a greater sense of unity within the organization (43). Similarly, Liu’s (2008) research highlighted the importance of interpersonal relationships and effective communication between managers and staff in the success of participatory management (45).
Despite the emphasis placed on human resources by various studies, some findings did not align with this perspective. Notably, Chang & Huang (2005) found that strategic human resource management does not necessarily have a significant impact on organizational performance, and no single HR management approach proved superior to others (46).
Overall, this scoping review reveals that human resources play a critical role in strengthening organizational capacity for implementing KT. To achieve effective readiness, medical universities should simultaneously focus on enhancing individual self-efficacy, developing participatory leadership, fostering staff motivation, improving interpersonal interactions, and engaging stakeholders.
These findings demonstrate that organizational readiness for knowledge translation is a complex and multidimensional phenomenon influenced by a combination of organizational and individual factors, including organizational climate, institutional support, change management, organizational context, and human resources. In alignment with international studies, these dimensions underscore that healthcare and academic organizations must pay strategic attention to such factors to successfully implement evidence-based change initiatives.
Based on the results of this study, a conceptual framework has been proposed for assessing organizational readiness to implement KT within Iranian medical universities. This framework may serve as a strategic tool for managers, planners, and health policymakers to focus on the identified key components and thus create the necessary conditions for effective KT processes. Although the core dimensions of organizational readiness are generally consistent across studies, the prioritization and weighting of each dimension vary depending on the cultural, social, and economic context. Therefore, integrating globally recognized indicators with locally adapted components can provide a comprehensive evaluation framework for higher education institutions in the health sector in Iran.Furthermore, strengthening transformational leadership, promoting a culture of innovation, expanding inter-organizational collaboration, and developing organizational change capacity require targeted investment and fundamental revisions in traditional academic and research structures. In this regard, medical librarians can play a pivotal role as knowledge intermediaries, evidence exchange facilitators, and advisors in clinical and educational decision-making. Ultimately, the conceptual model derived from this study can inform the development of practical and localized assessment tools in the KT domain and serve as an operational guide for policymakers and decision-makers in Iran’s health and medical education systems
The limitations of this study included restricted access to certain international databases due to sanctions (such as Scopus), which may have affected the comprehensiveness of the literature review. Additionally, the focus on type one medical universities limits the generalizability of the findings to other institutions and requires cautious interpretation. Among the strengths of this study were the systematic identification of key dimensions and components of organizational readiness for knowledge translation, which provided both a theoretical and operational framework for policymakers and educational managers. Furthermore, the integration of qualitative and quantitative methods contributed to a deeper extraction of concepts and enhanced the credibility of the findings.
Data Availability
All relevant data are within the paper however, any question or other file data is required you can contact us using the email address, upon reasonable request.
Acknowledgments
We thanks to clinical research development unit of rohani hospital.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Declarations
Ethics approval and consent to participate
This survey was carried out in accordance with the guidelines of the Declaration of Helsinki, was approved by the Ethics Committee of Kerman University of Medical Sciences (Ethics Code: IR.KMU.REC.1402.312).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests
References
- osadeghrad A, Isfahani P. 2021; Facilitators to health policy and management knowledge translation: A scoping review. Payesh (Health Monitor). 20(5):529-548 [in persian].
View at Publisher | View at Google Scholar - Kudyba SP. 2010. Healthcare informatics: improving efficiency and productivity: CRC Press;
View at Publisher | View at Google Scholar - Kalbarczyk A, Rao A, Alonge O. A 2021 mixed methods study to develop a tool to assess institutional readiness to conduct knowledge translation activities in low-income and middle- income countries. BMJ Open. 2021;11(10):2021-050049.
View at Publisher | View at Google Scholar - Jessani NS, Boulay MG, Bennett SC 2016. Do academic knowledge brokers exist? Using social network analysis to explore academic research-to-policy networks from six schools of public health in Kenya. Health policy and planning. 2016;31(5):600-11.
View at Publisher | View at Google Scholar - Weiner BJ. 2020 A theory of organizational readiness for change. Handbook on implementation science: Edward Elgar Publishing. 32-215.
View at Publisher | View at Google Scholar - Alizadeh M, Taghizadeh A, 2015editors. An overview of management systems deployment readiness assessment models. The third international conference on modern researches in management, economy and accounting; [in persian].
View at Publisher | View at Google Scholar - Edwards A, Zweigenthal V, Olivier J. 2019 Evidence map of knowledge translation strategies, outcomes, facilitators and barriers in African health systems. Health research policy and systems.;1714.-1:(1)
View at Publisher | View at Google Scholar - Mallidou AA, Atherton P, Chan L, Frisch N, 2018 Glegg S, Scarrow G. Core knowledge translation competencies: a scoping review. BMC health services research.;18(1):1-15.
View at Publisher | View at Google Scholar - Yousefi Nooraie R, Rashidian A, Nedjat S, Majdzadeh R, Mortaz Hedjri S, Etemadi A, 2009 et al. Promoting development and use of systematic reviews in a developing country. Journal of evaluation in clinical practice.;15(6):1029-1034[in persian]
View at Publisher | View at Google Scholar - Rashidian A. 2014Policy making challenges, and the need for introducing formal structures for evidence informed decision making in the health system. Hakim Research Journal.;16(3):258-261 [in persian].
View at Publisher | View at Google Scholar - Arksey H, O'Malley L. 2005 Scoping studies: towards a methodological framework, International Journal of Social Research Methodology; 8:19–32
View at Publisher | View at Google Scholar - Mosadeghrad AM, Tolouei Rakhshan Sh, Afshari A, Isfahani P. 2020 Health financing system indicators: A scoping review. Hakim Health Sys Res;20; 353-366
View at Publisher | View at Google Scholar - Kalbarczyk A, Rao A, Alonge OO. 2024 Determinants of factors affecting readiness of academic institutions to conduct knowledge translation in low-and middle-income countries. FRONTIERS IN PUBLIC HEALTH. 11:1302756.
View at Publisher | View at Google Scholar - Grandes G, Bully P, Martinez C, Gagnon M-P 2017;. Validity and reliability of the Spanish version of the Organizational Readiness for Knowledge Translation (OR4KT) questionnaire. IMPLEMENTATION SCIENCE. 12:1-11.
View at Publisher | View at Google Scholar - Attieh R, Gagnon M-P, Estabrooks CA, Légaré F, Ouimet M, Vazquez P 2014, et al. Organizational readiness for knowledge translation in chronic care: a Delphi study. BMC HEALTH SERVICES RESEARCH. 14:1-12.
View at Publisher | View at Google Scholar - Akram T, Lei S, Haider MJ, Hussain ST. 2020 The impact of organizational justice on employee innovative work behavior: Mediating role of knowledge sharing. Journal of Innovation & Knowledge.;5(2):117-129.
View at Publisher | View at Google Scholar - Fatemi SZ, Sadeghian S, Ganji SFG, Johnson LW. 2022;Do different genders' knowledge sharing behaviors drive different innovative behavior? The moderating effect of social capital. EUROPEAN JOURNAL OF INNOVATION MANAGEMENT. 25(2):592- 606.
View at Publisher | View at Google Scholar - Kakhki MK, Hadadian A, Joyame EN, 2020 Asl NM. Understanding librarians’ knowledge sharing behavior: The role of organizational climate, motivational drives and leadership empowerment. Library & Information Science Research.;42(1):100998.
View at Publisher | View at Google Scholar - Mbandi EM. 2020 Understanding the Relationship Between Perceived Organizational Support, Attitudinal Differences, and Knowledge Transfer Amongst Teleworkers at a US Federal Government Agency: Trevecca Nazarene University;.
View at Publisher | View at Google Scholar - Usmanova N, Yang J, Sumarliah E, Khan SU, Khan SZ2021;. Impact of knowledge sharing on job satisfaction and innovative work behavior: the moderating role of motivating language. VINE JOURNAL OF INFORMATION AND KNOWLEDGE MANAGEMENT SYSTEMS. 51(3):515-532.
View at Publisher | View at Google Scholar - Vandavasi RKK, McConville DC, Uen J-F, Yepuru P. 2020 Knowledge sharing, shared leadership and innovative behaviour: a cross-level analysis. INTERNATIONAL JOURNAL OF MANPOWER.;41(8):1221-1233.
View at Publisher | View at Google Scholar - Kuo Y-K, Kuo T-H, Ho L-A. Enabling innovative ability: knowledge sharing as a mediator. INDUSTRIAL MANAGEMENT & DATA SYSTEMS. 2014;114(5):696-710.
View at Publisher | View at Google Scholar - Bates R, Khasawneh S. 2005 Organizational learning culture, learning transfer climate and perceived innovation in Jordanian organizations. International journal of training and development.;9(2):96-109.
View at Publisher | View at Google Scholar - Banerjee P, Gupta R 2017;, Bates R. Influence of Organizational Learning Culture on Knowledge Worker?s Motivation to Transfer Training: Testing Moderating Effects of Learning Transfer Climate. Current Psychology. 36:606-617.
View at Publisher | View at Google Scholar - Strauss K, Griffin MA, Rafferty AE. Proactivity directed toward the team and organization: the role of leadership, commitment and role-breadth self-efficacy. Br J Manage. (2009) 20:279–91. 10.1111/j.1467-8551.2008.00590.x
View at Publisher | View at Google Scholar - Shea CM, Jacobs SR, . (2014) Esserman DA, Bruce K, Weiner BJ. Organizational readiness for implementing change: a psychometric assessment of a new measure. Implem Sci9:1–15.10.1186/1748-5908-9-7
View at Publisher | View at Google Scholar - Armenakis AA, Harris SG. 2002 Crafting a change message to create transformational readiness. JOURNAL OF ORGANIZATIONAL CHANGE MANAGEMENT. 15(2):169-183.
View at Publisher | View at Google Scholar - Armenakis A, Brown S, Mehta A. Organizational culture: Assessment and transformation. JOURNAL OF CHANGE MANAGEMENT. 2011;11(3):305-28.
View at Publisher | View at Google Scholar - Gagnon MP, Attieh R, Dunn S, Grandes G, Bully P, Estabrooks CA 2019., et al.. Future directions for the organizational readiness for knowledge translation (OR4KT) tool: response to recent commentaries. Int J Health Policy Manage. (2019) 8:315. 10.15171/ijhpm. 03
View at Publisher | View at Google Scholar - Gagnon MP, Labarthe J, Légaré F, Ouimet M, Estabrooks CA, Roch G, et al. 2011; Measuring organizational readiness for knowledge translation in chronic care. Implementation science : IS. 6(72):1748-5908.
View at Publisher | View at Google Scholar - Potter C, Brough R.. 2004. Systemic capacity building: a hierarchy of needs. Health Policy and Planning 19: 336–45.
View at Publisher | View at Google Scholar - El-Jardali F, Fadlallah R.. 2015. A call for a backward design to knowledge translation. International Journal of Health Policy and Management 4: 1–5.
View at Publisher | View at Google Scholar - Hawkes S, K Aulakh B, Jadeja N. et al. 2016. Strengthening capacity to apply health research evidence in policy making: experience from four countries. Health Policy and Planning 31: 161–70.
View at Publisher | View at Google Scholar - Holt DT, Armenakis AA, Feild HS, Harris SG. 2007 Readiness for organizational change: the systematic development of a scale. J Appl Behav Sci.;43(2):232–255. doi: 10.1177/0021886306295295.
View at Publisher | View at Google Scholar - Kitson AL, Rycroft-Malone J, Harvey G, McCormack B, Seers K, Titchen A. Evaluating the successful implementation of evidence into practice using the PARiHS framework: theoretical and practical challenges. Implement Sci. 2008;3:1. doi: 10.1186/1748-5908-3-1.
View at Publisher | View at Google Scholar - Kitson A, Harvey G, McCormack B. 1998 Enabling the implementation of evidence based practice: a conceptual framework. Qual Health Care.;7(3):149–158. doi: 10.1136/qshc.7.3.149.
View at Publisher | View at Google Scholar - Murunga VI, Oronje RN, Bates I, Tagoe N, Pulford J.. 2020. Review of published evidence on knowledge translation capacity, practice and support among researchers and research institutions in low- and middle-income countries. Health Research Policy and Systems 18: 16.37.
View at Publisher | View at Google Scholar - Weiner BJ, Belden CM, Bergmire DM, Johnston M. (2011) The meaning and measurement of implementation climate. Implem Sci. 6:1–12. 10.1186/1748-5908-6-78
View at Publisher | View at Google Scholar - Pearlmutter S. Self-efficacy and organizational change leadership. Adm Soc Work. (1998) 22:23–38. 10.1300/J147v22n03_02
View at Publisher | View at Google Scholar - Gagliardi AR, Webster F, Straus SE. (2015) Designing a knowledge translation mentorship program to support the implementation of evidence-based innovations. BMC Health Serv Res. 15:1–9. 10.1186/s12913-015-0863-7
View at Publisher | View at Google Scholar - Bandura A. (1986). Social Foundations of Thought and Action: A Social Cognitive Theory. Englewood Cliffs, NJ: Prentice-Hall;
View at Publisher | View at Google Scholar - Gist ME, Mitchell TR. . (1992) Self-efficacy: a theoretical analysis of its determinants and malleability. Acad Manage Rev17:183–211. 10.5465/amr.1992.4279530
View at Publisher | View at Google Scholar - Javad A. 2011.The rel+ationship between collaborative management and organizational climate with the effectiveness of middle school principals in Bandar Abbas city.
View at Publisher | View at Google Scholar - Rhoades L, Eisenberger R, Armeli S. 2001; Affective commitment to the organization: the contribution of perceived organizational support. Journal of Applied Psychology. 86(5):825.
View at Publisher | View at Google Scholar - Liu Y. 2008 Complexity science and participation in decision making among Taiwanese nurses. JOURNAL OF NURSING MANAGEMENT.;16(3):291-7.
View at Publisher | View at Google Scholar - April Chang WJ, Chun Huang T. 2005;Relationship between strategic human resource management and firm performance: A contingency perspective. INTERNATIONAL JOURNAL OF MANPOWER. 26(5):434-49.
View at Publisher | View at Google Scholar -
View at Publisher | View at Google Scholar
