

Case Report | DOI: https://doi.org/10.31579/2834-8761/080
Hormonal Upheavals for Healthy Young Women! “Premenstrual Syndrome & Heavy Menstrual Bleedings”
Public Health Consultant and Family Physician Bengaluru and Karnataka State Rural Development and Panchayat Raj University, GADAG, Karnataka, India 582101.
*Corresponding Author: K. Suresh, 70022, Altamura (Bari), Italy; Via Della Conciliazione, 65 Cap 74014 Laterza (Ta) Italy.
Citation: K. Suresh, (2025), Hormonal Upheavals for Healthy Young Women! “Premenstrual Syndrome & Heavy Menstrual Bleedings”, Clinical Endocrinology and Metabolism 4(2): 10.31579/2834-8761/080
Copyright: © 2025, K. Suresh. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 April 2025 | Accepted: 16 April 2025 | Published: 30 April 2025
Keywords: premenstrual syndrome (pms); heavy menstrual bleeding (hmb); menorrhagia; dysmenorrhea; premenstrual dysphoric disorder (pmdd); master’s in public health (mph); oestrogen; progesterone; aldosterone, oral contraceptive pill (ocp)
Abstract
Premenstrual Syndrome (PMS) and Heavy Menstrual Bleeding (HMB) are two conditions that can shatter the daily life young girls after menarche. Premenstrual Syndrome (PMS) is a condition characterized by changes in mood, emotions, physical well-being, and behaviour that occur between mid-cycle and menstruation. A range of 14.3% to 74.4% has been reported as the estimated prevalence of PMS in India. Heavy menstrual bleeding is an excessive menstrual blood loss that interferes with a woman’s physical, social, emotional or material quality of life. Both are explicit presentations of hormonal upheaval in young ladies. The exact cause or pathophysiology of PMS is yet to be understood but it appears to be multifactorial, with disturbances in aldosterone activity and Adolescent heavy menstrual bleeding (HMB) is commonly related to hypothalamic pituitary ovarian axis immaturity, which improves with age.
Studies show that menstrual disorders, at least one of the menorrhagia, dysmenorrhea, & PMS, are prevalent in a range of 60% to 80% of young Indian women. Specific treatment-seeking data varies, one study, reported that only a third of those with a menstrual complaint especially in Urban India sought treatment from a health facility, while others resorted to home remedies or self-medication. Materials and methods:
This article is outcome of small observational study of about 50 young ladies doing their post-graduation master’s in public health (MPH), with an average age of 24years, most of them in their 21-22 yrs. over three years between 2029-2022 and few other typical /atypical cases managed by Allopathy, Ayurveda and Homeopathy system of medical practices in India. Appropriate literature research adds to the epidemiology, and management practices.
Introduction
Premenstrual Syndrome (Pms) is a condition characterized by changes in mood, emotions, physical well-being, and behaviour that occur between mid-cycle and menstruation. A range of 14.3% to 74.4% has been reported as the estimated prevalence of PMS in India. PMS affects various aspects of daily life, of the young ladies, outside their home comforts for the first time when they opt for postgraduate studies. Its effects are social & interpersonal relationships, health-related quality of life, academic performance, & productivity. A higher prevalence of PMS is observed among rural girls compared to urban areas. PMS is associated with psychological & socio-demographic factors, like age, living region, & marital status [1]. The prevalence & severity of premenstrual syndrome (PMS) & premenstrual dysphoric disorder (PMDD) is associated with age, locality, food habits, obesity, stress, menorrhagia dysmenorrhoea and genetic influence. It is cyclical & exhibit 7- 10 days before menstruation onset, with relief shortly after. Up to 80 % women of reproductive age experience one/ more symptoms, with 50 % experiencing multiple symptoms & 20?cing severe symptoms [1,2]. Common symptoms are backache, fatigue, headache, nausea, Mastalgia (breasttenderness/pain), acne, insomnia, heightened appetite, diarrhoea & abdominal pain [3]. While Mastalgia, a most prevalent breast symptom observed in two thirds of the unmarried girls, severe forms affecting 10-20% classified as i) cyclic, ii) non-cyclic, & iii) extramammary. Diffuse & poorly localized cyclical breast pain need treatment [1,2]. The exact cause of PMS remains uncertain, multifactorial, with disturbances in aldosterone activity. Premenstrual Dysphoric Disorder (PMDD) is its most severe form, recognized as a psychiatric illness. The diagnostic criteria for PMS include the presence of at least 1 affective & 1 somatic symptom in the five days before the onset of menstruation. Genetic factors play a significant role in PMS. Mastalgia, a common symptom is reported in two thirds of the girls, with severe forms affecting 10-20% of them [1].
Heavy Menstrual Bleeding (Hmb) is an excessive menstrual blood loss that interferes with a woman’s physical, social, emotional or material quality of life. It poses a serious health issue causing impairment of quality of life and necessitate urgent medical attention. Experiencing heavy menstrual bleeding is associated with feeling tired during menstruation days [3]. It affects a significant portion of young girls ranging from 45% to 87.7% in India [5]. These two menstrual health issues are of a considerable concern among adolescent girls in India. Most Indian Gynaecologist manage PMS, & HBM with hormonal contraceptives, antidepressants, painkillers, though the first line of treatment is lifestyle modification. Both PMS and HMB often improve with treatment, but they must not be ignored, as they affect the quality of life & living on those days. This article is outcome of small observational study of about 47 young ladies doing their post-graduation master’s in public health (MPH), with an average age of 24years, most of them in their 21-22 yrs. over three years between 2029-2022.
Case Report 1. Mph scholars group study:
Methodology
: Following a session of Menstrual Cycle discrepancies & Public Health importance as a part of MPH course lesson, 2 volunteer girls one married and another unmarried were trained in each batch to take menstrual history. They were the first contacts in eliciting the symptom in casual discussions. The same methodology was used by all girls in a community survey of village school going girls of 8-18 years. The authors and the guide of study was approached by the scholars voluntarily if symptoms were bothering them. Surprisingly nearly two thirds of all (N=30) students did discuss one on one with the author. The reason for such large number seeking consultation with author though being male was his age of 75 years, professional experience and confidence they had in him due to comfort they have had in the type of participatory learning for action (PLA) process the author followed in all classes. Basic Socio-demographic characteristics were:
No of MPH scholars over 3 years of 2019-2022= 67, No of Female Scholars = 47
No Married=5, Unmarried=42, Hindu=35, Muslim=5, Others=7,
No responding in groups=07, No sharing information one on one=37,
non-responders=3
No followed up- for 2 yrs= 30, 3-4 yrs=12 yrs and 5 or more=2
Results:
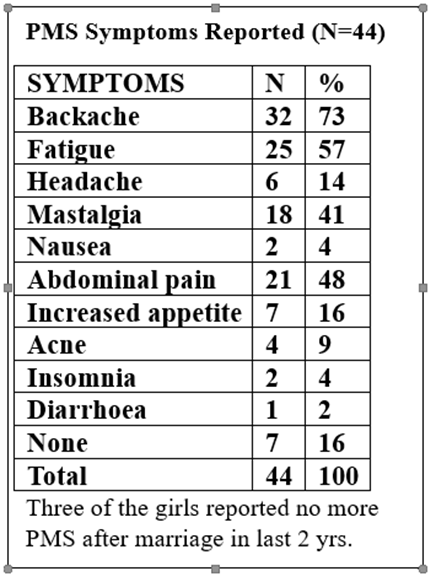
Overall Backache 3-5 days before the expected menses was the commonest symptom affecting nearly three fourths of the scholars followed unusual fatigue (25) and abdominal pain (21) & Mastalgia (18) among them even while sitting in the class on those days and one thirds of them found it difficult to concentrate in the class during those 3-5 days. Other symptoms in order of number suffered were increased appetite, headache, nausea, Acne, Insomnia and Diarrhoea, seven of them had no symptoms needing attention and all of them were married and 3 having 1-2 children. Four of them had consulted a Gynaecologists and were under hormonal therapy. Nearly 20 of the scholars took to lifestyle modification, including plenty of fluids herbal tea, timely meals regular exercises, Yoga or meditation & reported improvement.
Case report 2: pms managed by ayurvedic system:
A 15-year-old female patient reported to OPD with the complaints of headache, irritability, depression, extreme mood swings, lack of concentration, physically injuring herself, bloating 7-8 days prior to menstruation and it resolves with the onset of menstruation in first week of March 2024 to an Ayurvedic Medical College hospital. After physical & mental status assessment, using the diagnostic criteria she was diagnosed as Premenstrual Syndrome case. As per the protocol she was administered Kalyanaka Kashayam, Drakshadi Kashayam, Thalam with Ksheerabala for 3 months. Yoga Asanas and Pranayama’s were also advised. She is much better since last 6 months.
A Case of Pms Treated By Homeopathy: A female aged 23 years intern came to the OPD of a Govt. homoeopathic medical college hospital on 15/7/2024, with complaints of backache, swollen extremities, headache throbbing type of pain since 4 to 5 days. She said that this symptom came before 7 to 8 days prior to each of the menses. History revealed that since menarche she had to take allopathic medicines like antispasmodic and painkillers. She had her Menarche at 14 years of age, LMP: 20/6/2024, Cycle duration: 4/28 days. Menstrual bleeding was profuse, dark & clotted. Mother & an elder sister had no such problems. Her examination revealed i) BP: 120/ 70 mm of Hg ii) Pulse: 87 / min, iii) Weight: 55 kg iv) CVS: S1S2 Normal CNS: Conscious well oriented, RS: NA P/A: Soft and non –tender. Treatment: The case was repertorised with all symptoms and Folliculinum 30C were prescribed. In the next follow up (11/8/2024) the severity of symptoms had reduced. At the follow-up a placebo was prescribed. After the fourth follow up the severity of symptoms slightly increased that’s why few doses of Folliculinum 30 were repeated on 4/12/2024.After giving Folliculinum 30, patient was much better. Patient started Homoeopathic treatment from Aug 2024 and continued till March 2025, during this period the patient was not taking any allopathic medication for premenstrual syndrome and is happy.
Case reports of heavy menstrual bleeding (hmb):
Case Report1 Hmb Among Mph Scholars: Six of the MPH scholars did have HMB, four were already on oral contraceptive pills for 3-9monht and two more advised by the author were also put on Contraceptive pills making the menstrual cycles an-ovular and reducing the symptoms, they were advised to continue throughout the MPH course. Three of them have reported discontinuation of oral pills after marriage and the symptoms or resolved. Experiencing heavy menstrual bleeding was significantly associated with feeling tired or fatigue during the menstrual period and reporting worse self-rated physical health but was not associated with subjective wellbeing
A Case of Adolescent Menorrhagia Due to Decidual Cast After Oc Pills Treatment: A 13-year-old girl returned to the gynaecologic emergency room of a private medical college hospital after 25 days being on oral contraceptives for menorrhagia, brought for severe abdominal pain accompanied by moderate bleeding and followed by a decidual cast discharge of 10 × 9 × 2 cm, in the shape of a uterine cavity. On that day the patient had taken the fifth OC pill from the second package. On bimanual examination the uterus was soft, and vaginoscopy revealed a slightly dilated cervix with moderate bleeding from the uterine cavity. A transrectal ultrasound examination showed normal ovaries and 3-mm endometrium with a single, irregular, 9-mm echogenic structure localized in the left uterine corner. Pathologic examination of the cast revealed extensive decidual transformation of the endometrial stroma with atrophy of the glandular epithelium and suppurative and necrotic foci. Haemoglobin and hCG levels were 11 g/dL and 0.0 UA/mL, respectively. The patient was advised to complete the ongoing OC regimen and then allow withdrawal bleeding to occur. When the girl presented for the follow-up visit 4 weeks later, Uterus and ovaries on bimanual examination and scanning were normal, and the endometrial thickness was 4 mm with normal echogenicity. The girl was prescribed cyclic progestogen for three cycles. A follow-up after 6 months indicated resolution of the HMB.
Discussions:
Premenstrual Syndrome: Premenstrual Syndrome (PMS) is a condition characterized by changes in mood, emotions, physical well-being, and behaviour that occur between mid-cycle and menstruation. The diagnosis is based on the presence of at least one affective and one somatic symptom in the five days before the onset of menstruation after reviewing the adolescent’s symptoms recorded over three months. Affective symptoms include anxiety, irritability, angry outbursts, confusion, social withdrawal, or depression. Somatic symptoms include breast tenderness, abdominal bloating, headache, swelling of extremities, or changes in appetite. In Mastalgia, three types i) cyclic, ii) non-cyclic, &iii) extramammary most prevalent in two thirds of the unmarried girls, with severe forms affecting 10-20% of them. Treatment is necessary for, diffuse, & poorly localized cyclical breast pain [1].The exact cause of PMS remains uncertain and multifactorial, with hormonal fluctuations, disturbances in aldosterone activity, imbalances in the hypothalamic-pituitary-adrenal (HPA) axis, disturbed neurotransmitter secretion, functional hyperprolactinemia, dietary deficits of calcium, magnesium, and paradoxin, carbohydrate metabolism disturbances, and lifestyle factors like junk food intake, alcohol consumption, smoking, sedentary lifestyle, obesity, stress, and poor sleep habits. Genetic factors play a significant role in the pathogenesis of PMS, with oestradiol and serotonin being primary factors in genetically susceptible women predisposed to PMS. Oestradiol and serotonin are considered primary factors in genetically susceptible women predisposed to PMS [1,8]. A community based Cross-sectional study in schools of Anand District in State of Gujarat, India. Involving 1702 girls in the age group of 8–23 years who had achieved menarche reported the prevalence of moderate to severe PMS was 19.3% and PMDD was 4.6%. Almost all (94.8%) girls had at least one PMS symptom with 65.7% having moderate to severe symptoms. They found dysmenorrhoea in 71.2% girls and menorrhagia in 15.2%. Physical symptoms were reported by 53.5%, disruption of daily activities by 41.7%, while 25.1% had to miss school/college. Majority (81.3%) felt that PMS was a normal part of menstruation and 53.0% reported moderate to severe stress. Multivariate logistic regression model revealed older age, dysmenorrhoea, menorrhagia, high levels of stress and PMS in mother to be significantly associated with PMS. In addition to these, lower age at menarche and junk food significantly contributed to PMDD. [4] Research has shown that women with premenstrual syndrome often experience severe symptoms before their periods, significantly impacting their quality of life. PMS symptoms can lead to increased healthcare costs and diminished occupational productivity. A cross-sectional survey in Anand, Gujarat, revealed a 19.3% prevalence of PMS among 1,700 girls aged 8 to 23 [3]. A recent studies results show that the prevalence of Dysmenorrhea as highest (46% to 76%) among women, followed by PMS (40% to 71%), while PCOS (3% to 14.14%). The study found that irregular lifestyle, obesity, inadequate diet, age at marriage, family history, smoking, and place of residence factors is associated with menstrual disorders in India. As far as health-seeking for menstrual disorders is concerned, one-third of women sought treatment for menstrual disorders [5]. Most Indian Gynaecologist manage PMS, with hormonal contraceptives, antidepressants, painkillers, though the first line of treatment is lifestyle modification, including plenty of fluids, herbal tea, chamomile tea, a balanced diet, healthy nutrition, and timely meals. Pharmacotherapy like hormonal contraceptives, antidepressants, painkillers, diuretics, and SSRIs or SNRIs might be necessary in one thirds of the cases. Evening primrose oil (EPO) and vitamin E have shown to reduce breast pain and depression-related symptoms. Though PMS often improves with treatment, but not to be ignored, the school and Colleg going girls must be helped to improve their quality of life & living in those days by providing privacy, sanitary pads & toilets and counselling [1,9].
Management of pms in ayurveda system:
In Ayurveda Premenstrual syndrome is considered as a psycho neuro endocrine disorder of unknown aetiology, often noticed just prior to menstruation. The protocol of treatment includes administration of Kalyanaka Kashayam, Drakshadi Kashayam, Thalam with Ksheerabala for 3 months. Yoga Asanas and Pranayama’s were also advised [6].
Management of pms with homeopathic medicines:
Homeopathic practitioners use following medicines for various symptoms of PMS
1. Sepia/Chamomilla: these are the best homeopathic medicines for PMS, helps in curbing the extreme irritability and calms the mind.
2. Ignatia: This homeopathic remedy is used during PMS for treating depression and mood swings that women undergo.
3. Pulsatilla: During PMS, it is used for women who get extra sensitive towards everything and tend to get affected by the most insignificant matters which disrupt menstrual flow, accompanied by loss of thirst.
4. Lachesis: This medicine is used for women who suffer from body pain of PMS.
5. Conium/ Bryonia: Conium is the best homeopathic medicine for treating Mastalgia, characterized by breast tenderness during PMS, due to swelling, enlargement, hardness or pain or tenderness (pain on touching) in the breasts.
6.Carbo veg: This homeopathic medicine is used for the treatment of abdominal bloating in PMS.
Heavy menstrual bleeding (HMB): Heavy menstrual bleeding is defined as excessive menstrual blood loss that interferes with a woman’s physical, social, emotional or material quality of life. Puberty menorrhagia is excessive bleeding occurring between menarche and 19 years. Abnormal bleeding amounts to 50% of gynaecological visits in adolescent girls [7]. Heavy menstrual bleeding (HMB) poses a serious health issue causing impairment of quality of life and necessitate urgent medical attention [4]. A study aimed to detect the clinical indicators for common causes of HMB in adolescents and to assess the factors that influence clinicians' treatment choices, analysed electronic medical records of adolescents aged 10 to 18 with HMB from 2010 to 2022, a sample of 205 individual’s Clinical, laboratory, & treatment information was reviewed retrospectively. Nearly two thirds (63.9%) of patients were diagnosed with hypothalamic-pituitary-ovarian (HPO) axis immaturity, 13.7% with bleeding disorders (BD), and 12.2% with polycystic ovary syndrome (PCOS). The severity of bleeding or duration of bleeding at presentation among the three groups did not differ much. Patients with BD had lower haemoglobin (Hb) levels and required hospitalization more often. Among all participants, 34.6% received only iron supplements, 44.9% were treated with low-dose hormones, and 15.6% with high-dose hormones. Factors that led to the use of high-dose hormone therapy included lower Hb levels, treatment location (emergency room vs. clinic), and a history of multiple ER visits [4].Between Aug 2, 2021, and June 14, 2022, a Lancet study data reviewed 6626 women across ten cities (Meherpur and Saidpur, Bangladesh; Warangal, Narsapur, and Tiruchirappalli, India; Kathmandu, Nepal; Dakar, Senegal; Nairobi, Kenya; Kampala, Uganda; and Lusaka, Zambia), and 4828 women were included in the final analytic sample. In the pooled analytic sample, 2344 (48·6%) of 4828 women were classified as experiencing heavy menstrual bleeding. Experiencing heavy menstrual bleeding was significantly associated with feeling tired or short of breath during the menstrual period and reporting worse self-rated physical health but was not associated with subjective wellbeing [7]. A retrospective observational study of adolescents admitted for management of puberty menorrhagia in Kempe Gowda Institute of Medical Sciences, Bengaluru, from January 2017 to October 2021 from hospital records. They reported that amongst the 35 admitted, 42?longed to the age group 10-14 years. 62.8% presented with symptoms lasting less than 6 months. 20% presented with haemoglobin < 4>7 days of flow. Long blood flow duration was more prevalent in early than in late adolescence. 30.1% reported abundant blood loss. 66.8% had dysmenorrhea and no difference was observed between early and late adolescents. Menstrual cycles were shorter in early adolescence period [9].Adolescent heavy menstrual bleeding (HMB) is commonly related to hypothalamic pituitary ovarian axis immaturity, which improves with age. Acute adolescent HMB is rare. Medical treatment for adolescent HMB consists predominantly of hormonal contraceptives. Preparation choice depends upon patient preference, comorbidities & co-existing conditions.Although physicians tend to initiate high-dose hormonal treatments based on objective factors like Hb levels and hospitalization needs, clearer guidelines are required for starting low-dose hormonal therapies. Hence, there is a need for standardized protocols and practical implementation strategies for managing HMB in adolescents.
Conclusion:
Premenstrual Syndrome & Heavy Menstrual Bleeding in young women are explicit presentation of hormonal upheavalWhile Premenstrual Syndrome (PMS) is a condition characterized by changes in mood, emotions, physical well-being, and behaviour that occur between mid-cycle and menstruation, Heavy menstrual Bleeding (HMB) is defined as excessive menstrual blood loss that interferes with a woman’s physical, social, emotional or material quality of life. The exact cause or pathophysiology of PMS is yet to be understood but it appears to be multifactorial, with disturbances in aldosterone activity and Adolescent heavy menstrual bleeding (HMB) is commonly related to hypothalamic pituitary ovarian axis immaturity, which improves with age. Acute adolescent HMB is rare. Both conditions improve after marriage/ pregnancy and childbirth .Most Indian Gynaecologists prescribe oral contraceptive pill as needed or until the issue is resolved through natural course of marriage, pregnancy and childbirth, key events in a girls life that change hormonal imbalances.
References
- Hormonal Rollercoaster: Premenstrual Syndrome, Dr. Anita M, Ex AIIMS Obg. & Gynec. Faculty, New Delhi, https://www.emedinexus.com/47717/04/13/ 2025
View at Publisher | View at Google Scholar - Heavy menstrual bleeding in adolescents, Goker ETA, et.al, Int J Gynaecol Obstet. 2024 Dec 31. Doi: 10.1002/ijgo.16132. Epub ahead of print. PMID: 39739559.
View at Publisher | View at Google Scholar - Premenstrual syndrome in Anand District, Gujarat: A cross-sectional survey, Shruti V Kamat et.al, J Family Med Prim Care. 2019 Feb;8(2):640–647. Doi: 10.4103/jfmpc.jfmpc_302_18
View at Publisher | View at Google Scholar - Clinical Indicators & Treatment Preferences in Adolescents with HMB, https://www.medtalks.in/articles, 13 April 2025
View at Publisher | View at Google Scholar - Prevalence, risk factors &health-seeking behaviour of menstrual disorders among women in India, Puja Das et.al, https://Doi.org/10.1080/16549716.2024.2433331 24 Jan 2025
View at Publisher | View at Google Scholar - Ayurvedic management of Premenstrual Syndrome - A Case Study, Anisha A, Journal of Ayurvedic and Integrated Medical Sciences, https://jaims.in/jaims 03/28/2025
View at Publisher | View at Google Scholar - Prevalence of heavy menstrual bleeding and associations with physical health and wellbeing in Low- & Middle-Income countries, Sinharoy, Sheela S et al. https://www.thelancet.com/11/2023
View at Publisher | View at Google Scholar - Evaluation of cases of puberty menorrhagia requiring in-patient care, Reethu Varadarajan et.al, International Journal of Reproduction, Contraception, Obstetrics and Gynaecology, DOI: https://dx.doi.org/10.18203/2320-1770.ijrcog20221670
View at Publisher | View at Google Scholar - A study on menstruation of Indian adolescent girls in an urban area of South India, Shabnam Omidva et.al, J Family Med Prim Care. 2018 Jul-Aug;7(4):698–702. Doi: 10.4103/jfmpc.jfmpc_258_17
View at Publisher | View at Google Scholar - A case of unusual course of adolescent menorrhagia: decidual cast as a side effect of treatment
View at Publisher | View at Google Scholar - Anna Torres, https://www.fertstert.org/article/S0015-0282(09)02493-5/
View at Publisher | View at Google Scholar
