

Research Article | DOI: https://doi.org/10.31579/2834-8486/021
Dyslipidemia: Diabetes Lipid Therapies
- Rehan Haider *
Riggs Pharmaceuticals Department of Pharmacy, University of Karachi, Pakistan.
*Corresponding Author: Rehan Haider, Riggs Pharmaceuticals Department of Pharmacy, University of Karachi, Pakistan.
Citation: Rehan Haider., (2024). Dyslipidemia: Diabetes Lipid Therapies. International Journal of Clinical Therapeutics. 3(5); DOI:10.31579/2834-8486/021
Copyright: © 2024, Rehan Haider. Nguyen, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 October 2024 | Accepted: 22 October 2024 | Published: 30 October 2024
Keywords: dyslipidemia; diabetes; lipid therapies; ldl cholesterol; hdl cholesterol; cholesterol absorption inhibitors; cardiovascular complications; blood sugar control; monitoring
Abstract
Dyslipidemia refers to a bizarre lipid profile characterized by increased cholesterol and/or triglyceride levels and decreased levels of excess density lipoprotein (HDL) cholesterol. It is not unusual comorbidity in people with diabetes and poses a high risk for cardiovascular disease (CVD). Powerful control of dyslipidemia in diabetes requires a complete method that includes way-of-life adjustments and pharmacological interventions. manner of existence modification, including adopting a wholesome phase weight reduction plan and increasing physical interest, plays a critical role in coping with dyslipidemia. A diet low in saturated fats, trans fats, and LDL cholesterol, blended with an emphasis on consuming high-fiber components and omega-3 fatty acids, can enhance lipid profiles. Ordinary exercise can decrease HDL cholesterol levels and weight loss, in addition to supporting dyslipidemia management. At the same time, my way of life changed with diabetes, and pharmacological treatment plans were prescribed regularly. Statins are the cornerstone of dyslipidemia treatment because of their ability to lower low-density lipoprotein (LDL) cholesterol levels. In humans with diabetes, statin remedies have been suggested to reduce the risk of CVD, regardless of the baseline lipid degrees. Different lipid-lowering dealers, including ezetimibe, bile acid sequestrants, and PCSK9 inhibitors, can be used as upload-on remedies to enhance lipid profiles. In recent years, modern formulations of antidiabetic tablets have been shown to have beneficial effects on lipid parameters in patients with diabetes. Sodium-glucose co-transporter-2 (SGLT-2) inhibitors and glucagon-like peptide-1 receptor agonists (GLP-1 RAs) have cardiovascular and lipid-lowering effects. SGLT-2 inhibitors reduce LDL cholesterol and triglyceride levels simultaneously with LDL-HDL cholesterol production, whereas GLP-1 RAs generally reduce triglyceride and LDL cholesterol levels.
Introduction
The association between diabetes and heart disease was first described more than a century ago. Two decades later, in 1906, it was hypothesized that this association was caused by atherosclerosis. The importance of diabetes as a cardiovascular disease (CVD) risk factor was established following the Framingham Study, which was subsequently confirmed by other landmark studies [1,2]. The magnitude of diabetes as a CVD risk factor is substantial, with an increase in the cardiovascular risk. Many guidelines regard diabetes as coronary heart disease (CHD) risk equivalent [3 – 5]. This concept was originally based on a Finnish cohort [6], which showed a comparable risk of CHD outcomes, such as myocardial infarction (MI) and CHD death, between subjects with type 2 diabetes mellitus (T2DM) for > 10 years and those with established CHD (Figure 40.10 ).
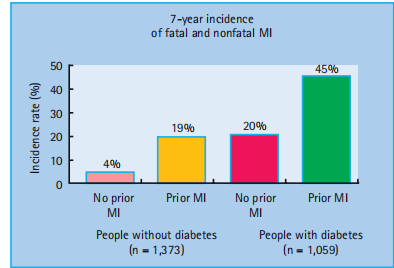
Figure 40:10 Equivalence of cardiovascular risk in patients with previous coronary heart disease (CHD) and those with diabetes. MI, myocardial infarction. Reproduced from Haffner et al. [6] , with permission from Massachusetts Medical Society.
This was still apparent after adjusting for known risk factors such as age, sex, hypertension, total cholesterol, and smoking. The Organization to Assess Strategies for Ischemic Syndromes (OASIS) study showed that patients with diabetes and no previous CVD have the same long-term morbidity and mortality as patients with established CVD but no diabetes after hospitalization for unstable coronary artery disease (CAD) [7]. However, there is a wide variation in the rate of CHD in diabetes, which depends on the population studied, the duration of diabetes, and existing risk factors [8,9]. This equivalence has not been confirmed in a subsequent study, and it seems less valid in older subjects, where those with existing CHD have a greater risk than non-CHD patients with diabetes [9,10]. Most of the literature on CVD risk and diabetes considers only T2DM. Although people with type 1 diabetes mellitus (T1DM) are at an increased risk of CVD [11,12], no study has specifically examined whether subjects with T1DM have a CVD risk that is comparable to or higher than that of those with T2DM. T1DM may be associated with a high risk of premature CVD. In a cohort of 292 patients with T1DM followed for 20 – 40 years, the cumulative mortality rate from CAD was 35% years by 55 years of age [11]. As T1DM mostly presents at an earlier age, it remains more difficult to assess and compare, but the rates of CVD increase at all ages [13]. Concomitant CVD risk factors also differ according to diabetes type. For example, patients with T1DM have a two - to three-fold increase in the risk of developing CHD and stroke later in life. This risk was notably higher in patients with nephropathy. Other markers of CVD risk in people with diabetes include diabetic retinopathy, autonomic neuropathy, erectile dysfunction, micro albuminuria, and proteinuria [14]. In general, individuals with diabetes have a two - to fourfold CVD risk compared with those without diabetes [15]. Although guidelines do not recommend formal CVD risk estimation in patients with diabetes because of the significant risk these patients already have and the tendency of the Framingham algorithm to underestimate the risk in this group, clinicians may still opt to estimate the risk by employing various risk calculators, of which the UK Prospective Diabetes Study (UKPDS) is the most commonly used [16]. It should be noted, however, that these risk calculators predict risk with variable accuracy [17]. As all methods of CVD risk estimation suffer from distinct limitations, clinical judgment remains necessary to accurately assess risk and select and titrate the appropriate treatment [18,19].
Cardiovascular disease risk factors in diabetes
Glucose
A hazard continuum exists throughout a broad glucose attention range that includes individuals without diabetes, with the hazard of CVD being lowest when fasting blood glucose is 4 – 4.9 mmol/L [20 – 22]. Regardless of the proper - setup affiliation between blood glucose and atherosclerosis, few studies have investigated the development of cardiovascular outcomes through a reduction in blood glucose. In T1DM, the Epidemiology of Diabetes Interventions and Complications (EDIC) examination [23] which followed topics after the completion of the Diabetes Management and Headaches Trial located that glucose reduction is associated with a long-term benefit for cardiovascular headaches, which have become the most effective years after recruitment. In T2DM, 10 - 12 months follow-up records from the UKPDS in-depth glucose therapy showed lengthy-term benefits and bio-effects on macro-vascular consequences [24]; but, in contrast to the microvascular benefits, chance discounts for MI and death from any motive had been determined most effective with prolonged post-trial compliance with - up (figure 40.11.). these results cautioned that stepped-forward glucose management may result in a bigger cardiovascular danger reduction in patients with T1DM than among those with T2DM, which is consistent with the results of a previous meta-analysis. Furthermore, neither the current action in Diabetes and Vascular disorders: Preterax and Diamicron Modified launch controlled assessment (develop) [25] nor the action to govern Cardiovascular danger in Diabetes (ACCORD) [26] trials, every which includes an extra of 10 000 participants, could not display a significant
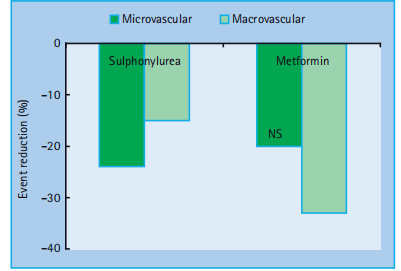
Figure 40:11 Results of the UK Prospective Diabetes Study (UKPDS) at 10 years follow - up. Reproduced from Holman et al. [24], with permission from Massachusetts Medical Society
beneficial effect on CVD outcome whilst targeting close to - regular glucose tiers in T2DM as determined by using an HbA 1c < 6>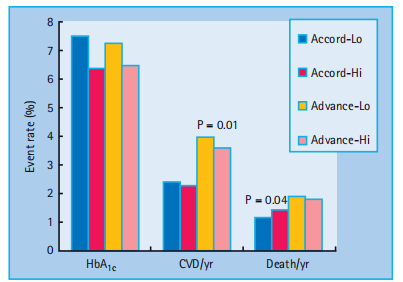
Figure 40:12 Effects of improved diabetes control to an HbA 1c < 6>
Dyslipidemia compared with hyperglycemia, focused dyslipidemia, has established plenty extra effective in preventing the macro vascular headaches of diabetes; however, for many years the benefits of intervention on lipoproteins as cardiovascular hazard factors in diabetes had been unsure. The fundamental cause was that humans with diabetes were excluded from trials of lipid-decreasing cures. Therefore, no statistics exist from early studies of bile acid sequestrants, fibrates, or nicotinic acidThe motives for the extra CVD hazard in diabetes are several and vary in the components associated with lipid abnormalities visible in diabetes. Greater glycation of lipoproteins has direct effects on lipoprotein metabolism, as glycated lipoproteins are handled otherwise via lipoprotein receptors, especially of the scavenger institution, as a consequence of atherogenesis [29]. More desirable glycation also amplifies the outcomes of oxidative stress on lipoproteins and therefore influences both T1DM and T2DM [30]. The period of diabetic dyslipidemia refers to the lipid abnormalities normally observed in men and women with T2DM and is synonymous with atherogenic dyslipidemia [31,32]. It is characterized by accelerated triglyceride-rich remnant lipoproteins(hypertriglyceridemia), small, dense LDL particles, and low high-density lipoprotein (HDL) cholesterol concentrations. Several factors are likely responsible for diabetic dyslipidemia: the effects of insulin on liver Apolipoprotein production, downregulation of lipoprotein lipase (LPL) as opposed to hepatic lipase, increased cholesteryl ester transfer protein (CETP) activity, and peripheral effects of insulin on adipose tissue and muscle.
Low-density lipoprotein cholesterol
LDL cholesterol has been identified as the primary target for lipid-lowering therapies. Analysis of the UKPDS showed that LDL cholesterol was the strongest risk factor for CHD in this population, followed by HDL cholesterol was the second strongest [33]. Even relatively modern studies discouraged recruitment or restricted entry to patients with hypercholesterolemia and reasonable glycemic control (HbA 1c < 8 xss=removed>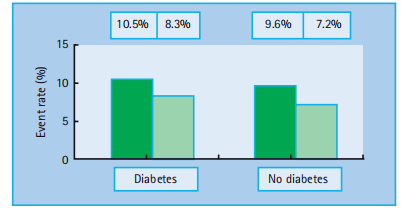
Figure 40:13 Comparison of the effects of reducing low density lipoprotein (LDL) cholesterol on cardiovascular events in patients with and without diabetes. Reproduced from Cholesterol Treatment Triallists Collaborators. Lancet 2005; 366 :1267 – 1278, with permission from Elsevier.
sequestrants. The cholesterol absorption inhibitor, ezetimibe, works by lowering the upper intestinal cholesterol concerning surrogate marker measurements and pointers of potentially detrimental effects [44]. Two ongoing trials, the Improved Reduction of Outcomes: Victorian Efficacy International Trial (IMPROVE-IT), in which simvastatin plus ezetimibe was compared to a placebo, and the Study of Heart and Renal Protection (SHARP) trial, in which simvastatin plus ezetimibe was compared to a placebo, will hopefully provide answers to these questions.
Low-density lipoprotein subfraction.
LDL elegance accommodates a heterogeneous population of debris [45]. LDL is heterogeneous in terms of lipid composition, fee, density, particle length, and shape. The sizes of LDL particles fall between those of large triglyceride-enriched very-low-density lipoprotein (VLDL) particles and dense and small protein-rich HDL. Furthermore, this small dense LDL debris can be more atherogenic than could be suspected by using their concentration alone, because in vitro and cell way of life studies propose that they are more readily oxidized and glycated. Oxidized LDL provides LDL cholesterol to atherosclerotic plaques in an unregulated manner via uptake by macrophages and is elevated in diabetes [46]. Every other component is the fatty acid composition of the LDL particles. Linoleic acid is the principal polyunsaturated fatty acid in LDL particles and its levels are elevated in diabetes. This may be due to a decreased interest in the insulin-sensitive enzyme, 5 α - desaturase. There is a robust correlation between linoleic acid inside LDL particles and the propensity of LDL particles to oxidize. Out-of-control diabetes results in extended free radical formation, which in turn results in expanded oxidation. LDL debris is smaller and denser and brings rather less LDL cholesterol in line with the particles. Estimation of the LDL cholesterol may also, therefore, be misleading as there can be greater LDL debris for any cholesterol concentration. huge numbers of studies, inclusive of the Quebec Cardiovascular examination [47], have confirmed the association of small dense LDL with CVD which pronounced that men with small dense LDL particles had a multiplied danger of CAD in comparison with guys with ordinary-sized LDL debris, impartial of LDL cholesterol, triglyceride, and the total LDL cholesterol: HDL cholesterol ratio; however, no potential studies have specifically examined whether altering particle length profiles effects benefits aerobic vascular activities even though evaluation of the Veterans Affair's high-Density Lipoprotein LDL cholesterol Intervention Trial (VA - HIT) take a look at and recommend some functions for this mechanism [48]. even with powerful LDL cholesterol treatment, the residual risk of similar cardiovascular occasions remains excessive, emphasizing the importance of enhancing other abnormalities and different CVD danger elements typically observed in these Patients Triglycerides
The reason for elevated triglyceride levels in diabetes is complex; however, because of this derangement, it is recommended that diabetes should no longer be called mellitus but as an alternative lipid [49]. Defects in insulin motion and hyperglycemia can result in adjustments in the plasma lipoproteins of patients with diabetes. Instead, especially in the case of T2DM, obesity and insulin-resistant metabolic disarray, which is the basis of this form of diabetes, could result in lipid abnormalities and one-of-a-kind hyperglycemia [32]. This molecular interplay between lipid and carbohydrate metabolism has led to what is probably termed a " lipocentric " view of the pathogenesis of insulin resistance and T2DM [50]. As fatty acids have a primary function in insulin sensitivity, obesity, and T2DM, it follows that the main disturbance in lipoprotein metabolism in diabetes is discovered inside triglyceride-rich lipoproteins, stemming from abnormalities in chylomicron synthesis and clearance [51]. Triglycerides (additionally called triacylglycerol) are fashioned from a single molecule of glycerol combines with 3 fatty acids and constitutes a heterogeneous organization of molecules that are regularly measured collectively as the " own family " of analytes [52]. Accelerated serum triglyceride levels are associated with an increased risk of atherosclerotic events [53,54]. As high serum triglyceride levels are related to unusual lipoprotein metabolism, as nicely as with other cardiovascular risk elements inclusive of weight problems, insulin resistance, diabetes, and coffee stages of HDL cholesterol, it turns into a greater difficult to differentiate between purpose and impact and established hypertriglyceridemia as an independent component of aerobic vascular hazards. Hypertriglyceridemia has no apparent effect on atherosclerotic vascular ailments, making it difficult to prove that extended triglyceride levels are a risk factor [55].However, numerous meta-analyses have reported that triglycerides are an independent risk factor for CHD [54,56,57].
The two major components of plasma triglycerides are exogenous (i.e., from nutritional fat) carried in chylomicrons and endogenous (from the liver) carried in VLDL debris. In capillaries within fats and muscular tissues, these lipoproteins and chylomicrons are hydrolyzed with the aid of LPL into free fatty acids. LPL is activated by Apolipoprotein C - II, cleaving the triglyceride center and liberating free fatty acids, which can be oxidized through muscle for energy or stored in adipose tissue for future use and inhibited by the action of Apolipoprotein C - III [58]. In ordinary clinical practice, hypertriglyceridemia is the most frequent lipoprotein abnormality associated with uncontrolled diabetes mellitus. These mechanisms include expanded manufacturing or absorption or a decreased catalog list (in particular, due to decreased LPL pastime). Liver Napoli lipoprotein B manufacturing (the principal protein component of VLDL and LDL) levels are increased in patients with T2DM. is in a roundabout way introduced approximately by elevated lipolysis, which takes place in adipose tissue, a consequence of insulin resistance and/or insulin deficiency. The expanded lipolysis outcomes in an expanded fatty acid release from fat cells with an increase in fatty acid shipping to the liver. Research in tissue cultures, animal experiments [59], and humans [60] has suggested that fatty acids modulate liver Apolipoprotein B secretion.Microsomal triglyceride transfer protein (MTP) assembles into chylomicrons in the intestine and VLDL particles in the liver. MTP is increased in the intestines of subjects with diabetes . Cholesterol absorption also appears to be adversely affected in patients with diabetes. The Niemann – Pick C1 - like 1 protein, which plays a critical role in cholesterol absorption, is increased in individuals with diabetes. ATP-binding cassette transporters ABC - G5 and ABC - G8 dimerize to form a functional complex that is necessary for the efflux of dietary cholesterol and non-cholesterol sterols from the intestine and liver. These proteins are reduced in diabetes in both Liver and intestine. LPL is an insulin-dependent enzyme responsible for converting lipoprotein triglycerides to free fatty acids. It has several other activities relating to lipid and carbohydrate metabolism . Both patients with T1DM and T2DM have reduced LPL activity which is further suppressed by adipose-derived cytokines such as tumor necrosis factor α(TNF-α ), and interleukin 6 (IL - 6) [32]. Statins are the mainstay of lipid management based on their efficacy in lowering LDL cholesterol, but their effects on components of atherogenic dyslipidemia associated with T2DM are modest, reducing triglycerides by 15 – 30% and increasing HDL cholesterol by less than 10%. There is no clear consensus on the benefits of directly targeting hypertriglyceridemia . As interventions usually affect both triglycerides and high-density lipoprotein (HDL) cholesterol, it becomes more difficult to distinguish between individual benefits.
Fibrates
The " fibrate " class of lipid-lowering drugs is useful for lowering elevated triglyceride or non - HDL cholesterol levels, as these agents, which act on the peroxisomal proliferator-activated receptor α (PPAR α ), increase lipoprotein lipase activity, reduce Apolipoprotein C - III, and may increase HDL cholesterol or decrease fibrinogen . Despite this, clinical trials of these drugs have reported mixed results in general, and most early trials recruited Only a few patients have diabetes. The VA-HIT study evaluated the potential benefits of gems in Brazil in 2531 men with acute MI. Patients with relatively low LDL cholesterol ( < 3 xss=removed>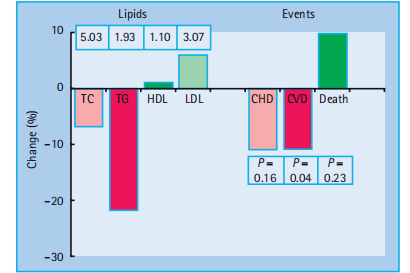
Figure 40:14 Reductions in mortality, coronary heart disease (CHD) and cardiovascular events with fenofibrate therapy in the FIELD study. HDL, high density lipoprotein; LDL, low density lipoprotein; TC, total cholesterol; TG, triglycerides. Reproduced from Keech et al. [70] , with permission from Elsevier.
Niacin
Nicotinic acid (niacin) is another drug used to cope with the combination of hypertriglyceridemia and occasional HDL–LDL cholesterol. Owing to its favorable effects on LDL cholesterol, it is known as the "huge-spectrum" lipid drug . Nicotinic acid is the first lipid-lowering agent to show a significant reduction in cardiovascular activity but is no longer associated with mortality. The Coronary Drug undertaking randomized 3908 men with previous MI to either nicotinic acid or placebo . most crucial CHD activities, non-deadly MI, and cerebrovascular occasions had been decreased, however, there has been no effect on mortality; but, within the 15-year post-trial have a look at - up, almost 9 years after the termination of the trial, mortality from all causes was 11% lower within the nicotinic acid institution . several prolonged - period medical studies with niacin have thought about that tested a reduction in CHD activities and mortality simultaneously when utilized in combination with extraordinary lipid-editing pills, which consist of colestipol (a bile acid sequestrant) , fire and statins . Unfortunately, niacin has been hampered by its side effects, particularly flushing, although strategies exist to reduce these side effects and hyperglycemia . No long-term outcome trials of niacin in patients with diabetes have been conducted yet. Furthermore, niacin adversely affects glycemic control. This effect was related to the dose of nicotinic acid. The study of the effect of extended-release niacin on diabetic dyslipidemia found that, at week 16, the HbA 1c did not change significantly in the 1 g group; in the 1.5 g group, there was an increase from 7.2% (55 mmol/mol) to 7.5% (58 mmol/mol) [80]. Wider variations are seen in clinical practice. Analysis of data from the Coronary Drug Project showed that regardless of how patients were grouped, niacin appeared as effective in lowering cardiovascular outcomes in patients with hyperglycemia, as in normoglycemia patients (Figure 40.15 ) The guidelines on the use of niacin in patients with diabetes are conflicting. The current position statement from the American Diabetes Association (ADA) suggests the use of nicotinic acid as an option in treating lipoprotein fractions other than LDL cholesterol. It has been reported that only modest changes in glucose occur and that these changes are generally amenable to the adjustment of diabetes therapy.
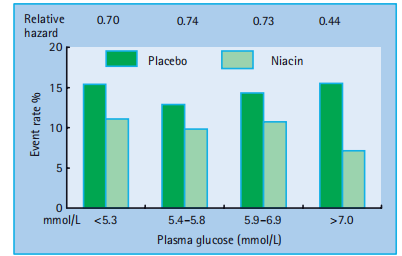
Figure 40:15 Reduction in coronary heart disease in patients with a fasting plasma glucose > 7 mmol/L from a post hoc analysis of the Coronary Drug Project. Reproduced from Canner et al. [81] , with permission from Excerpta Medica.
A previous statement discouraged its routine use, as does the recent National Institute for Health and Clinical Excellence (NICE) guidelines for the Management of Diabetes in England and Wales . Large-scale outcome studies are currently in progress. The Atherothrombosis Intervention in Metabolic Syndrome with Low HDL Cholesterol/high triglyceride and Impact on Global Health The outcomes (AIM-HIGH) were reported in 2011 . The large Oxford-based outcome trial with extended-release niacin/laropiprant (an inhibitor of prostaglandin receptor D1 which reduces the flushing) The Heart Protection Study 2 - Treatment of HDL to Reduce the Incidence of Vascular Events (HPS2 - THRIVE) , includes 28 000 patients with cardiovascular disease or at high risk of developing it, including a pre-specified subgroup of 6000 with diabetes, and is scheduled to report in 2013.
Other triglyceride-reducing agents
scientific Trial In macro-vascular events (PROACTIVE) have a look at, which added pioglitazone to the modern-day treatment of patients with T2DM, confirmed that treatment with pioglitazone changed into associated with discounts in major atherosclerotic occasions as defined in Primary secondary endpoints [94]. The differential results on lipid profiles may additionally explain the differences between these two pills on CVD consequences, as reported in the latest meta-analyses (Figure 40.16)
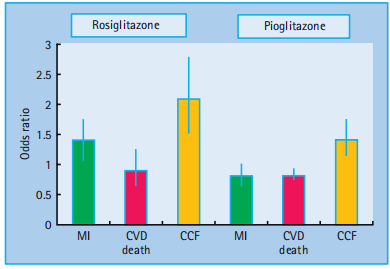
Figure 40:16 Effects of thiazolidinedione drugs on coronary heart disease (CHD) in trials using rosiglitazone and pioglitazone. CCF, congestive cardiac failure; CVD, cardiovascular disease; MI, myocardial infarction. Reproduced from Singh et al. JAMA 2007; 298 :1189, with permission from the American Medical Association.
Some of the different current interventions reduce triglycerides secondary to movement to decrease weight . Orlistat has been proven to prevent the development of diabetes inside the Xenical in the prevention of diabetes in overweight topics (XENDOS) take a look at [98], and sibutramine and rimonabant (earlier than their suspension) showed benefits for lipids in patients with metabolic syndrome and diabetes. Rimonabant had a non - significant benefit on coronary atherosclerosis, as assessed by intra vascular ultrasound, in keeping with its lipid results . High-density lipoprotein LDL cholesterol.
Analogous to LDL, HDL comprises a heterogeneous population of particles. Inverse dating of HDL cholesterol levels and atherosclerotic CVD afforded a robust biological foundation for the broadly well-known speculation that HDL is atheroprotective Experimental studies that have included restrained paintings in humans have shown that HDL has several distinct but potentially overlapping atheroprotective functions. These include the well-known reverse cholesterol transport , as well as reductions in oxidative stress and innate immune inflammation . More HDL-associated proteins are involved in immune/inflammatory functions than in lipid transport and metabolism, suggesting a fundamental role of HDL in innate immunity Several factors may account for the decreased HDL cholesterol levels in diabetes CETP-mediated exchange of VLDL triglycerides for HDL cholesteryl esters is accelerated in the presence of hypertriglyceridemia . The clinical laboratory measures the cholesterol component of HDL; the substitution of triglycerides for cholesteryl ester in the core of the HDL particle leads to a decrease in the measurement of HDL cholesterol. Triglyceride, but not cholesteryl ester, is a substrate for plasma lipases, especially hepatic lipase, which converts HDL into smaller particles that are more rapidly cleared from the plasma. Precursors of advanced glycation end-products (AGEs) can also impair reverse cholesterol transport by HDL. As opposed to LDL cholesterol lowering, therapies to intervene to raise HDL cholesterol have proven to be " not that simple. " Some HDL therapies may reduce CVD without changing HDL cholesterol concentration . The Intra vascular An Ultrasound Study (IVUS) of the effects of 5 weekly infusions of hyper-functional Apolipoprotein A - 1 (apoA - 1) Milano produced significant regression of coronary atherosclerosis after 3 months. In contrast, in the Investigation of Lipid Level Management to Understand Its Impact on Atherosclerotic Events (ILLUMINATE) trial, which investigated the CETP inhibitor, torcetrapib, in 15 000 patients, HDL cholesterol increased by 72% and LDL cholesterol decreased by 25%, although this trial was terminated early as the treatment arm had an increase in major cardiovascular events by 25% and death from cardiovascular causes by 40%, possibly related to the hypertensive properties of this particular molecule.
Guidelines vary when it comes to treatment targets for HDL
cholesterol levels, mostly because there is currently no evidence-based intervention . The Joint British Societies Guidelines and NICE argue that there is no treatment target for HDL cholesterol, as it is only modestly altered and is not independent of changes in other lipid variables in clinical trials . Furthermore, there are no drugs available yet that independently alter HDL cholesterol. The American Heart Association and the ADA suggest lowering triglycerides to below 1.7 mmol/L (150 mg/dL) and raising HDL to more than 1.15 mmol/L (40 mg/dL) In women, an HDL cholesterol goal of 0.3 mmol/L (10 mg/dL) higher than this should be considered.
Future drug developments and drug targets
Drugs that target exogenous or endogenous pathways of cholesterol metabolism may prove useful in the future . These include Niemann – Pick C1 - like 1 Protein inhibitors, novel PPAR agents, and MTP inhibitors. Interventions that regulate fatty acid synthesis may be beneficial. Stearoyl-coenzyme A desaturase 1 catalyzes the synthesis of monounsaturated fatty acids and has emerged as a key metabolic regulator . Recent studies in human and animal models have highlighted that modulation of stearoyl-coenzyme A desaturase 1 activity by dietary intervention or genetic manipulation strongly influences several facets of energy metabolism and affects the susceptibility to obesity, insulin resistance, diabetes, and hyperlipidemia. HDL mimetic therapies may also be beneficial. Other CETP inhibitors are still under investigation . Although numerous drug classes have been devised, many, such as torcetrapib, have recently failed in late phase III trials even after showing good initial results for lipids in human and animal models. Other drugs, such as rimonabant, have shown unfavorable side effects, which has led to the suspension of marketing in the European Union. Given the importance of atherosclerosis as a cause of morbidity and mortality in diabetes, numerous therapeutic approaches are in development, This will require systematic evaluation through endpoint clinical trials to validate their effects in animal models or surrogate markers.
Research Method:
A complete literature review was conducted to collect the facts from this dialogue. PubMed, MEDLINE and other relevant databases were searched using the key phrases "dyslipidemia," "diabetes," and "lipid remedies." Studies published between 2010 and 2021 were included in this meta-analysis. Both randomized controlled trials and meta-analyses were selected for the analysis. The selected studies evaluated the efficacy and protection of diverse lipid-reducing agents in patients with diabetes and dyslipidemia.
Results:
The outcomes of the literature review indicated that numerous lipid-decreasing therapies have established efficacy in treating dyslipidemia in people with diabetes. The following key findings were obtained:
Statins are the primary therapy for dyslipidemia in patients with diabetes. Numerous studies have shown their effectiveness in reducing low-density lipoprotein cholesterol (LDL-C) levels and the risk of cardiovascular disease. They also validated some blessings in improving glycemic management and reducing irritation marker levels.
Ezetimibe, a cholesterol absorption inhibitor, is often used in combination with statins to reduce LDL-C levels. Studies have shown that the addition of ezetimibe to statin therapy offers additional LDL-C reduction, which can also result in progressive cardiovascular effects. PCSK9 inhibitors: Pro protein convertase subtilisin/kexin type 9 (PCSK9) inhibitors have emerged as a singular class of lipid-lowering marketers. They paint by blocking PCSK9, thereby increasing the range of LDL and ensuing a huge discount in the LDL-C stages. Clinical trials have validated its efficacy in reducing LDL-C levels and cardiovascular events in patients with diabetes.
Discussion:
The findings of this study highlight the importance of lipid-lowering treatment plans for the management of dyslipidemia in patients with diabetes. Statins remain the cornerstone of remedies, owing to their validated efficacy and cardiovascular benefits. mixture, along with statins and ezetimibe, is frequently recommended to achieve similar LDL-C reduction. PCSK9 inhibitors have shown promise as adjunct remedies for patients with persistent excessive LDL-C levels despite maximal statin therapy.
It is critical to bear in mind the protective profile of lipid-reducing healing procedures, mainly in diabetic patients who might also have comorbidities and take a couple of medicinal drugs. Statins are generally well tolerated, but are associated with muscle-associated side effects or elevations in liver enzymes. Ezetimibe is generally safe and well-tolerated when used in a mixture of statins. PCSK9 inhibitors have been proven to have a good protection profile in scientific trials, but their high cost remains a barrier to their sizeable use.
Conclusions
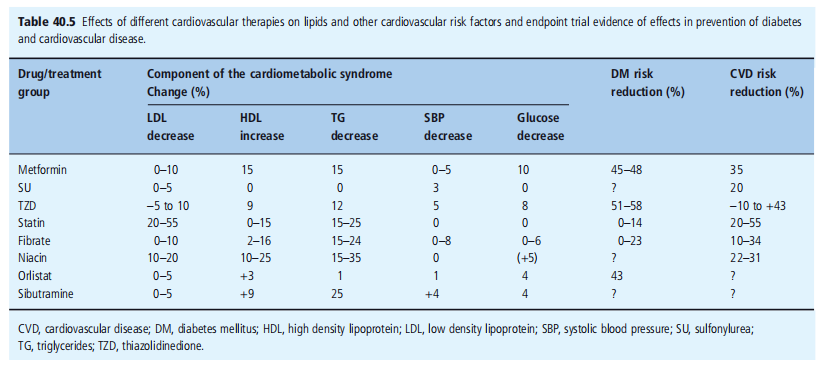
CVD is a common complication of diabetes mellitus. Up to 80% of all people with diabetes die of complications. Lifestyle intervention is both effective and paramount to Prevention and treatment of diabetes and dyslipidemia. Statins have revolutionized preventive cardiovascular medicine and formed the foundation of therapeutic lipid interventions (Figure 40.17 ). Abnormalities in lipids and lipoproteins represent only one factor among the several that are responsible for the increased risk in individuals with diabetes (Table 40.5 ). Therefore, multifactorial interventions are required, which reduce events and mortality by 50% (Figure 40.18 )
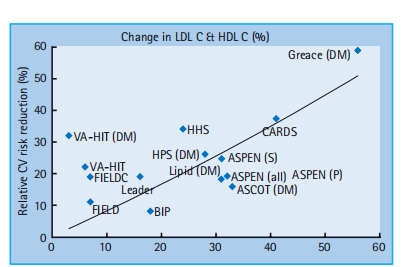
Figure 40:17 Comparative effects of different lipid lowering drugs on cardiovascular disease (CVD) in patients with diabetes. ASPEN, Atorvastatin Study for the Prevention of Coronary Heart Disease Endpoints in Non-Insulin-Dependent Diabetes Mellitus; BIP, Bezafibrate Infarct Prevention; CARDS, Collaborative Atorvastatin Diabetes Study; FIELD, Fenofibrate Intervention and Event Lowering in Diabetes; FIELDc, FIELD study (corrected data); GREACE; Greek Evaluation of Atorvastatin in Coronary Events; HHS, Helsinki Heart Study; HPS, Heart Protection Study; LEADER, Lower Extremity Arterial Disease Event Reduction; LIPID, Lipid Intervention with Pravastatin in Ischaemic Disease; VA-HIT, Veterans Affairs High Density Lipoprotein Cholesterol Intervention Trial; DM, diabetes sub-group; P, primary prevention subgroup; S, secondary prevention subgroup; HDL C, high density lipoprotein cholesterol; LDL C, low density lipoprotein cholesterol. Reproduced from Wierzbicki AS. Diab Vasc Dis Res 2006; 3 :166 – 171, with permission from Medinews.
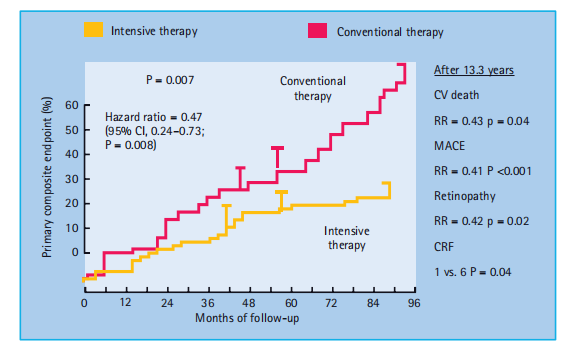
Figure 40: 18 Effects of improved multiple risk factor intervention on mortality and cardiovascular events in diabetes.
CABG, coronary artery bypass graft; CV, cardiovascular; MI, myocardial infarction; PAD, peripheral arterial disease; PC, percutaneous coronary intervention. Data from Gaede et al. N Engl J Med 2003; 348 :383 – 393 and Gaede et al. N Engl J Med 2008; 358 :580 – 591
Acknowledgment
The crowning glory of this research challenges could no longer be feasible without the contributions and guidance of many individuals and agencies. we’re deeply grateful to all those who performed a position in the achievement of this mission We also thank My Mentor [. Naweed Imam Syed Prof. Department of Mobile Biology at the College of Calgary and Dr. Sadaf Ahmed Psychophysiology Lab University of Karachi for their helpful input and guidance throughout this study. Their insights and understanding had been instrumental in shaping the direction of this challenge
Declaration of interest
I, at this second, declare that: I haven’t any pecuniary or another private hobby, direct or oblique, in any dependence that raises or can also boost a war with my duties as a supervisor of my workplace control.
Conflicts of Interest
The authors declare that they have no conflict of interest
Financial support and sponsorship
No Funding was received to assist with the preparation of this manuscript.
References
- Kannel WB, McGee DL. (1979).Diabetes and cardiovascular disorder: the Framingham study. JAMA: 241: 2035 – 2038.
View at Publisher | View at Google Scholar - Kannel WB, McGee DL. (1979). Diabetes and glucose tolerance as threat factors for cardiovascular sickness in the Framingham study. Diabetes Care; 2: – 126.
View at Publisher | View at Google Scholar - (2001). professional panels on the detection of elevated atherosclerotic cardiovascular disease (ASCVD) risk: executive summary of the 0.33 document of the National Cholesterol Education Program (NCEP). JAMA; 285: 2486-2497.
View at Publisher | View at Google Scholar - Graham I , Atar D , Borch - Johnsen ok , Boysen G , Burell G , et al. (2007). Fourth Joint assignment pressure of the EU Society of Cardiology and one-of-a-kind societies on cardiovascular ailment prevention in medical exercise (constituted via representatives of 9 societies , and invited specialists). Eur J Cardiovasc Prev Rehabil; 14 (Suppl 2 ): S1 – 113.
View at Publisher | View at Google Scholar - (2005). British Cardiac Society, British excessive blood stress Society, Diabetes UK, et al. JBS 2: the Joint British Societies ’ tips for prevention of cardiovascular sickness in scientific exercise. coronary heart; 91 (Suppl 5): 1 – 50.
View at Publisher | View at Google Scholar - Haffner SM , Lehto S , Ronnemaa T , Py ö r ä l ä good enough , Laakso M . (1998). Mortality from coronary coronary coronary heart disease in subjects with kind 2 diabetes and in Non diabetic subjects with and without advanced myocardial infarction. N Engl J Med; 339 : 229 – 234 .
View at Publisher | View at Google Scholar - Malmberg k , Yusuf S , Gerstein HC , Brown J , Zhao F , et al. (2000). effect of diabetes on prolonged-period evaluation in patients with volatile angina and non - Q - wave myocardial infarction: effects of the OASIS (corporation to assess strategies for Ischemic Syndromes) circulate; 102: 1014 – 1019.
View at Publisher | View at Google Scholar - Howard BV, nice LG, Galloway JM, Howard WJ, Jones K, et al. (2006). Coronary coronary coronary heart disorder danger equivalence in diabetes was based on concomitant risk factors. Diabetes Care; 29: 391 – 397.
View at Publisher | View at Google Scholar - Evans JM, Wang J, Morris ad. (2002). Assessment of cardiovascular chance between patients with kind 2 diabetes and people who had had a Myocardial infarction: bypass sectional and cohort studies, Br Med J; 324: 939 – 942.
View at Publisher | View at Google Scholar - Simons l. A., Simons J. (1998). Diabetes and coronary heart disease N Engl J Med; 339 : 1714 – 1715
View at Publisher | View at Google Scholar - Krolewski AS , Kosinski EJ , Warram JH , Leland OS , Busick EJ, et al. (1987). Magnitude and determinants of coronary artery disease in Juvenile-onset insulin-established diabetes mellitus. Am J Cardiol; 59: 750 – 755.
View at Publisher | View at Google Scholar - Jensen T , Borch - Johnsen ok , Kofoed - Enevoldsen A , Deckert T . (1987). Coronary coronary heart disorder in younger kind 1 (insulin - structured) diabetic patients with and without diabetic nephropathy: incidence and chance elements. Diabetologia; 30: 144 – 148.
View at Publisher | View at Google Scholar - Soedamah - Muthu SS, Fuller JH, Mulnier HE, Raleigh VS, Lawrenson RA, et al. (2006). All-reason mortality fees in sufferers with kind 1 diabetes mellitus as compared with a non-diabetic population from the United Kingdom Trendy Practice Studies Database. 1992 – 1999. Diabetologia; 49: 660 – 606.
View at Publisher | View at Google Scholar - 14 Mogensen CE. Microalbuminuria predicts medical proteinuria and Early mortality in maturity-onset diabetes. N Engl J Med 1984 ; 310: 356 – 360.
View at Publisher | View at Google Scholar - Kannel WB. (1985). Lipids, diabetes, and coronary heart ailments: insights from the Framingham Study. Am Heart J; one hundred ten: 1100 – 1107.
View at Publisher | View at Google Scholar - Stevens RJ, Kothari V, Adler AI, Stratton IM. (2001). The UKPDS danger engine: a model for the threat of coronary heart sickness in type II diabetes (UKPDS 56). Clin Sci (Lond); one hundred and one: 671 – 679.
View at Publisher | View at Google Scholar - Coleman RL, Stevens RJ, Retnakaran R, Holman RR. (2007). Framingham, score, and DECODE threat equations no longer offer dependable vehicle cardiovascular risk estimates in patients with type 2 diabetes. Diabetes Care; 30: 1292 – 1293.
View at Publisher | View at Google Scholar - Viljoen A. (2008). Cardiovascular danger estimation: Making feel of the number. Int J Clin Pract; 62: 1300 – 1303.
View at Publisher | View at Google Scholar - Reynolds TM and Twomey PJ. Wierzbicki AS. (2004). Concordance evaluation of coronary danger scores: implications for cardiovascular risk display. Curr Med Res Opin; 20: 811 – 818.
View at Publisher | View at Google Scholar - (1999). Twenty DECODE had a look at the group. Is fasting glucose sufficient to define diabetes? Epidemiological statistics from 20 EU studies Ecu Diabetes Epidemiology Organisation. Diabetes Epidemiology: Collaborative Analysis of Diagnostic Standards in Europe. Diabetologia; 42: 647 – 654.
View at Publisher | View at Google Scholar - Meigs JB, Nathan DM, Wilson PW et al, (1998). Singer DE. Metabolic risk factors continuously worsen across the spectrum of non-diabetic glucose tolerance. The Framingham Offspring appeared. Ann Intern Med; 128: 524 – 533.
View at Publisher | View at Google Scholar - Levitan EB, track Y, Ford ES, Liu S. (2004). Is non-diabetic hyperglycemia a hazard for cardiovascular disease? Meta-analysis of potential studies Arch Intern Med; 164: 2147 – 2155.
View at Publisher | View at Google Scholar - Nathan DM, Cleary PA, Backlund JY, Genuth SM, Lachin JM, et al. (2005). In-depth diabetes treatment and cardiovascular disorders in patients with type 1 diabetes. N Engl J Med; 353: 2643 – 2653.
View at Publisher | View at Google Scholar - Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. (2008). 10-year comply with in-depth glucose control in type 2 diabetes. N Engl J Med; 359: 1577 – 1589.
View at Publisher | View at Google Scholar - Patel A, MacMahon S, Chalmers J, Neal B, Billot L, et al. In-depth blood glucose manipulation and vascular outcomes in patients with type 2 diabetes mellitus N Engl J Med 2; 3:2560 – 2572.
View at Publisher | View at Google Scholar - Gerstein HC, Miller ME, Byington RP, Goff DC Jr, et al. (2008). In-depth glucose decrease in type 2 diabetes. N Engl J Med; 358: 2545 – 2559.
View at Publisher | View at Google Scholar - Dluhy RG and McMahon GT. (2008). intensive glycemic manipulation in the ACCORD, and strengthened the trials. N Engl J Med; 358: 2630 – 2633.
View at Publisher | View at Google Scholar - Cefalu WT. (2008). Glycemic targets and cardiovascular disorders. N Engl J Med; 358: 2633 – 2635.
View at Publisher | View at Google Scholar - Beauchamp MC, Michaud SE, Li L, Sartippour MR, Renier G. (2004). Superior glycation inhibits the stimulatory effect of glucose on macrophage lipoprotein lipase expression. J Lipid Res; 45: 1749 – 1757.
View at Publisher | View at Google Scholar - Lyons TJ, Jenkins AJ, et al. (1997). Lipoprotein glycation and its metabolic consequences. Curr Opin Lipidol; eight: 174 – 108
View at Publisher | View at Google Scholar - Durrington PN. (1999). Diabetic dyslipidemia. Baillieres excellent Pract Res Clin Endocrinol Metab; 13: 265 – 278.
View at Publisher | View at Google Scholar - Goldberg IJ. (2001). Diabetic dyslipidemia: causes and effects. medical overview 124. J Clin Endocrinol Metab; 86: 965 – 971.
View at Publisher | View at Google Scholar - Turner RC, Millns H, Neil HA, et al. (1998). Risk elements for coronary artery ailment in non-insulin-based diabetes mellitus: uk potential Diabetes Study (UKPDS:23). Br Med J; 316: 823 – 828.
View at Publisher | View at Google Scholar - (1994). Scandinavian Simvastatin Survival Study (4S) Investigators. A randomized trial of cholesterol lowering in 4444 patients with coronary heart disease: The Scandinavian Simvastatin Survival Study (4S). Lancet; 344: 1383 – 1389
View at Publisher | View at Google Scholar - Peralak, Pedersen T.R., Kekshus J., Faergeman O., Olsson A.G., Thorgeirsson G. (1997). Simvastatin improves low-density lipoprotein cholesterol lowering Prognosis in diabetic patients with coronary artery disease: a subcenter evaluation of the Scandinavian Simvastatin Survival Study (4S). Diabetes Treatment; 20:614-620.
View at Publisher | View at Google Scholar - Sacks FM, Tonkin AM, Shepherd J, Braunwald E, Cobb S, et al. Hawkins the effect of pravastatin on coronary events in the subcommittee of KM et al is described using coronary risk factors: pravastatin function Associated work. 2000 according to the flow; 102: 1893 - 1900
View at Publisher | View at Google Scholar - Colhoun HM, Betteridge DJ, Durrington PN, Hitman GA, Neil HA, et al. (2004). Primary prevention of back cardiovascular disease Combination with atorvastatin for type 2 diabetes in atorvastatin joint study Diabetes Screening (Playing Cards): Multicenter Randomized Placebo-control test. Lancet; 364:685–696.
View at Publisher | View at Google Scholar - (2002). Cardiovascular Safety (MRC/BHF Investigators) MRC/BHF coronary heart A look at the safety of lowering LDL cholesterol with simvastatin in 20,536 high-risk groups: A randomized, placebo-controlled trial. window; 360:7-22.
View at Publisher | View at Google Scholar - Collins R, Armitage J, Parish S, et al. (2003). Coronary heart protection view co-organizations. Coronary heart protection MRC/BHF LDL cholesterol lowered by simvastatin in 5963 diabetic patients: A randomized placebo-controlled trial. The Lancet; 361: 2005- 2016.
View at Publisher | View at Google Scholar - Knopp R.H., d'Emden M., Smilde J.G., Pocock S.J. (2006). Efficacy and Safety Oral atorvastatin for Cardiovascular Disease Prevention Type 2 Diabetes Related Topics: Atorvastatin for Prevention Endpoints of Coronary Heart Disease in the Absence of Insulin Diabetes Mellitus (OSIN). Diabetes Treatment; 29:1478 - 1485.
View at Publisher | View at Google Scholar - Wanner S., Crane W., Marz W., Olszewski M., Mann J. F., et al. (2005). Atorvastatin in patients with type 2 diabetes undergoing hemodialysis. N Engl J Med; 353:238-248.
View at Publisher | View at Google Scholar - Kearney P.M., Blackwell L., Collins R., Keach A., Simes J., et al. (2008). Efficacy of LDL-C-lowering agents in 18,686 diabetic patients in 14 randomized statin trials. The Lancet; 371:117 — 125
View at Publisher | View at Google Scholar - Rossebo AB, Pedersen TR, Boman good enough, Brudi P, Chambers JB, (2008). Egstrup good enough, et al. In-intensity lipid reduction with simvastatin and ezetimibe in aortic stenosis. N Engl J Med ; 359 : 1343 – 1356 .
View at Publisher | View at Google Scholar - Wierzbicki AS. (2008). Muddy Waters: More stormy SEAS for Ezetimibe. Int J Clin Pract; 60-: 1470–1473.
View at Publisher | View at Google Scholar - Austin MA. (2000). Triglycerides, small, dense low-density lipoproteins, and Atherogenic lipoprotein phenotype. Curr Atheroscler Rep; 2: 200–207.
View at Publisher | View at Google Scholar - Scheffer PG , Teerlink T , Heine RJ . (2005). The scientific significance of the physicochemical properties of LDL in type 2 diabetes. Diabetologia; 48: 808 – 816.
View at Publisher | View at Google Scholar - St - Pierre AC, Cantin B , Dagenais GR , St - Pierre AC , Cantin B, et al. (2005). Low-density lipoprotein subfraction and the prolonged-time period hazard of ischemic coronary heart disorder in guys: 13 - one-year follow-up records from Quebec Cardiovascular were examined. Arterioscler Thromb Vasc Biol; 25: 553 – 559.
View at Publisher | View at Google Scholar - Otvos JD, Collins D, Freedman DS, Shalauvova I, Schaefer EJ, et al. (2006). Low-density lipoprotein and high-density lipoprotein particle subclasses assume coronary activities and are favorably modified via gems Brazil remedy within the Veterans Affair's excessive - Density Lipoprotein Intervention Trial. circulation; 113: 1556 – 1563.
View at Publisher | View at Google Scholar - Shafrir E, Raz I. (2003). Diabetes mellitus or lipidaemia Diabetologia; 46: 433 – 440.
View at Publisher | View at Google Scholar - Savage DB, Petersen KF, Shulman GI, et al. (2007). Disordered lipid metabolism and the pathogenesis of insulin resistance. Physiol Rev; 87: 507 – 520.
View at Publisher | View at Google Scholar - Kahn SE, Hull RL, Utzschneider KM. (2006). Mechanisms linking obesity for insulin resistance and type 2 diabetes. Nature; 444: 840 – 846.
View at Publisher | View at Google Scholar - Thienpont LM, Van uk AP, De Leenheer AP. (2002). Reference size systems of scientific chemistry. Clin Chim Acta; 323: 73 – 87.
View at Publisher | View at Google Scholar - McBride P. (2008). Triglycerides and threats to coronary artery disorders. Curr Atheroscler Rep; 10: 386 – 390.
View at Publisher | View at Google Scholar - Sarwar N , Danesh J , Eiriksdottir G , Sigurdsson G , Wareham N , et al. (2007). Triglycerides and the danger of coronary heart illness 10,158 incident times among 262,525 participants in 29 Western ability studies. motion; 115: 450 – 458.
View at Publisher | View at Google Scholar - Austin MA, McKnight B, Edwards KL, Bradley CM, McNeely MJ, et al. (2000). Cardiovascular illness mortality inside the familial paperwork of hypertriglyceridemia: a 20 - yr potential have a look at. pass; one 0 one: 2777 – 2782.
View at Publisher | View at Google Scholar - Austin MA, Hokanson JE, Edwards KL. (1998). Hypertriglyceridemia is a Cardiovascular risk factors. Am J Cardiol; eighty-one: 7 B – 12 B.
View at Publisher | View at Google Scholar - Assmann G , Schulte H , von EA . (1996). Hypertriglyceridemia and elevated lipoprotein(a) are risk elements for essential coronary sports in the center -elderly guys. Am J Cardiol; 77: 1179 –1184.
View at Publisher | View at Google Scholar - Grundy SM. (1998). Hypertriglyceridemia, atherogenic dyslipidemia, and metabolic syndrome. Am J Cardiol; 81- 18 B – 25 B.
View at Publisher | View at Google Scholar - Taghibiglou C, Carpentier A, Van Iderstine SC, Chen B, Rudy D, et al. (2000). Mechanisms of hepatic very low-density lipoprotein overproduction in insulin resistance: proof for higher lipoprotein meeting, reduced intracellular ApoB degradation, and improved microsomal triglyceride switch protein in a fructose-fed hamster version. J Biol Chem; 275: 8416 – 8425.
View at Publisher | View at Google Scholar - Lewis GF, Uffelman KD, Szeto LW, Weller B, et al. (1995). Interaction between unfastened fatty acids and insulin during the intense manipulation of very-low-density lipoprotein manufacturing in humans. J Clin Invest; 90 5: 158 – 166.
View at Publisher | View at Google Scholar
