

Research Article | DOI: https://doi.org/10.31579/2834-5142/103
Dengue in End-Stage Renal Disease Patients on Hemodialysis: Evaluating Clinical Profiles and indicators of critical outcome during a Major Outbreak in Bangladesh
- Masrura Jabin 1
- , Mamun Mostafi 2*
- Shaila Rahman 3
- Ahmed Shahriar 4
- Saad bin Alamgir 4
- Tanvir Chowdhury 4
1Associate Professor, and Head Department of Nephrology, Gonoshasthaya Samaj Vittik Medical College and Hospital.
2Professor Emeritus, Gonoshasthaya Samaj Vittik Medical College and Hospital.
3Associate Professor, Department of Medicine, Shaheed Monsur Ali Medical College, Uttara, Dhaka.
4Registrar, Department of Nephrology, Gonoshasthaya Samaj Vittik Medical College and Hospital.
*Corresponding Author: Mamun Mostafi, Professor Emeritus, Gonoshasthaya Samaj Vittik Medical College and Hospital.
Citation: Masrura Jabin, Mamun Mostafi, Shaila Rahman, Ahmed Shahriar, Saad bin Alamgir, et.al., (2025), Dengue in End-Stage Renal Disease Patients on Hemodialysis: Evaluating Clinical Profiles and indicators of critical outcome during a Major Outbreak in Bangladesh. I Journal of Clinical Nephrology. 4(2); DOI:10.31579/2834-5142/103
Copyright: © 2025, Mamun Mostafi. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 April 2025 | Accepted: 16 April 2025 | Published: 23 April 2025
Keywords: Dengue, clinical profile, outcome, ESRD, severe dengue
Abstract
Introduction: Dengue has become prevalent in over 100 nations across the WHO Regions. Asia bearing approximately 70% of the worldwide disease burden experiencing the most severe impact. Bangladesh, an endemic zone, witnessed its largest-ever dengue outbreak marked by atypical seasonality and a 0.5% case fatality rate. This study, aimed to investigate the clinical presentation, outcomes, frequency of warning signs and severe dengue and indicators of critical outcome in patients of end-stage renal disease (ESRD) undergoing maintenance hemodialysis (MHD)
Methods: An observational study was conducted at Gonoshasthaya Nogor Hospital, Dhaka, Bangladesh, during the dengue outbreak from June to December 2023, included ESRD patients who had been taking MHD for at least 3 months and were admitted to the hospital with dengue infection. Appropriate statistical tests were done.
Results: 28 cases of dengue-infected ESRD patients on MHD were included in the study. 53.6% were male and 46.4 % were females. Mean age was 41.18+14.003 years (minimum 18 years, maximum 74 years). The comorbidities were notable, hypertension (92.86%), diabetes mellitus (32.14%), ischaemic heart disease (10.71%) and glomerulonephritis (7.14%). Fever was the most common clinical feature (92.86%), then loose motion (46.42%), breathlessness (35.71%), vomiting (32.14%), and shock (32.14%). A significant proportion (75%) of patients presented with WHO-defined warning signs upon hospital admission. The mortality was 32.14%. In the univariate model altered consciousness, shock, leukocytosis (>12000/cmm), thrombocytopenia (<45000/cmm) and hypoalbuminaemia (<25gm/L) were the predictors of death. In the multiple regression model, by the Forward Wald method, only shock was found to be the independent predictor of death. It is important to highlight that 32.14% of dengue-infected ESRD patients developed severe dengue, and all of them died.
Conclusion:
The study highlights the vital importance of early recognition of warning signs in ESRD dialysis patients to prevent severe complications related to dengue. The high mortality rate emphasizes the urgent need for targeted interventions and careful management strategies within this high-risk population.
Introduction
Dengue fever is a mosquito-borne disease that affects millions of people in tropical and subtropical regions annually. The World Health Organization (WHO) estimates that over 3.9 billion individuals residing in these areas are at risk of dengue infection. Dengue has become prevalent in over 100 nations across the WHO Regions. Asia bearing approximately 70% of the worldwide dengue burden experiencing the most severe impact. [1]
While dengue is a known endemic disease in Bangladesh, the present upsurge in dengue cases is atypical due to its unusual seasonal onset and the rapid rise, in contrast to last years. The Ministry of Health and Family Welfare of Bangladesh reported a total of 283593 laboratory-confirmed dengue cases and 1425 dengue related deaths from 1 January to 7 November 2023, with a case fatality rate (CFR) of 0.5% this makes it the largest outbreak of dengue fever reported [2].
The spectrum of clinical manifestations associated with dengue is broad, ranging from no symptom and self-limiting illness to life-threatening forms of the disease. In 2009, the WHO reclassified dengue fever. The updated classification categorizes dengue into two main groups: non-severe and severe dengue (SD). Non-severe dengue is further subdivided into two types: dengue with warning signs and dengue without warning signs. Early recognition of severe dengue is of great importance for reducing dengue-related mortality. [1,3].
Several factors contribute to develop severe dengue. Though, secondary infection is a risk factor, distinguishing primary from secondary dengue infection early on is challenging, especially in endemic regions with limited medical setups. Comorbidities or pre-existing medical conditions, represent another significant predictor of severe dengue. Other than diabetes, hypertension, coronary artery disease, and chronic obstructive airway disease/bronchial asthma; renal insufficiency emerged as a substantial risk factor linked to heightened disease severity and increased mortality. Patients with chronic kidney disease (CKD) who are infected with dengue display unusual clinical manifestations, deteriorating renal function, and poorer clinical outcomes [4].
Aim of the study: This study aimed to identify predictors associated with clinical outcomes in dengue, with a particular focus on patients with end-stage renal disease taking hemodialysis. By gaining a comprehensive understanding of these predictors, this research seeks to improve patient triage, enhance the quality of care, and ultimately reduce dengue-related mortality.
Materials and methods
This was an observational study conducted at a Gonoshasthaya Nogor hospital, Dhaka, Bangladesh from June to December 2023, a major outbreak of dengue occurred in Bangladesh during this period. All ESRD patients taking maintenance hemodialysis for at least three months, who were admitted to the hospital with dengue infection fulfilling the inclusion and exclusion criteria were enrolled in the study. Written informed consent was taken from all patients. The observational period started from the first day of admission and ended after discharge or death whichever came earlier. Patients aged less than 18 years were excluded from the study.
Case definitions: A case of dengue fever was defined as a clinical illness with either positive NS1 antigen or positive IgM dengue antibody. Clinical features of dengue fever were defined as an acute febrile illness with two or more of the following: headache, myalgia, arthralgia/ bone pain (break-bone fever), rash, gastrointestinal (GIT) manifestations: nausea, vomiting, diarrhoea (seen in recent outbreaks), haemorrhagic manifestations (mild, unusual haemorrhage), leukopenia, thrombocytopenia and rising hematocrit. The warning signs include symptoms like abdominal pain or tenderness, persistent vomiting, clinical fluid accumulation, mucosal bleeding, lethargy or restlessness, liver enlargement greater than 2 cm, altered consciousness and an increase in hematocrit concurrent with a rapid decrease in platelet count. Severe dengue was defined as one of the following: 1) severe plasma leakage (shock/fluid accumulation with respiratory distress), 2) severe bleeding and 3) severe organ involvement (ALT/AST > 1000 I/U or CNS involvement or heart or other organ involvement). [5]
Statistical analyses
Fisher’s Exact test was used to compare baseline characteristics of dengue patients with and without warning signs. Binary logistic regression models were utilized to determine the risk factors associated with the development of severe dengue. Initially, univariate logistic regression analyses were conducted to calculate crude odds ratios (cORs) and their 95% confidence intervals (CIs). Subsequently, multivariate logistic regression was performed to adjust for potential confounders, with results presented as adjusted odds ratios (aORs) and corresponding 95% CIs.A p-value of less than 0.05 was regarded as statistically significant. All analyses were conducted using the Statistical Package for the Social Sciences for Windows (SPSS) version 25.0 (SPSS Inc., Chicago, IL, USA).
Results
28 ESRD patients on maintenance hemodialysis were included in the study. The mean age was 41.18+14.003 years (minimum 18 years, maximum 74 years). Most of the patients (16, 57.2%) were within the age group of 20-39 years. 15 (53.6%) were males and 13 (46.4 %) were females. Common comorbidities were hypertension (26, 92.86%), diabetes mellitus (9, 32.14%), ischaemic heart disease (3, 10.71%) and glomerulonephritis (2, 7.14%) (Table 1)
Characteristics |
|
Age (in years) mean+SD | 41.18+14.003 |
Male (n, %) |
|
Co-Morbidities (n, %) | 53.6% |
Hypertension | 26 (92.86%) |
Diabetes mellitus | 9 (32.14%) |
Ischaemic heart disease | 3 (10.71%) |
Glomerulonephritis | 2 (7.14%) |
HCV (+) | 2 (7.14%) |
HBs Ag (+) | 1 (3.57%) |
SLE | 1 (3.57%) |
Latent TB | 1 (3.57%) |
Table 1: Demographic characteristics and comorbidities of total study subjects (n=28)
SD=standard deviation, HCV=hepatitis C virus, HBsAg (+) = hepatiitis B positive, SLE=systemic lupus erythematosus, TB=tuberculosis. 92.86% of cases had fever. Loose motion (46.4%), shock (32.1%), vomiting (31.2%), breathlessness (35.71%%), bleeding (21.4%), abdominal pain (14.3%) and altered consciousness (14.3%) were also observed frequently. 7.1% of patients had cough. (Figure 1)
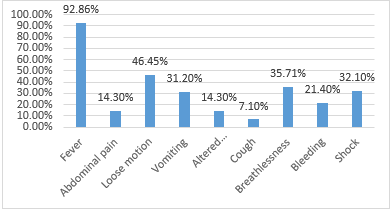
Figure 1: Clinical features observed in the study participants (n=28) *not mutually exclusive
21 (75%) patients had warning signs. 9 (32.1%) cases had severe dengue. Patients with ischaemic heart disease, SLE and ≥2 comorbidities had a relatively higher frequency of presenting with warning signs. However, it was not statistically significant. Patients presenting with warning signs at presentation had a higher frequency of plasma leakage, severe dengue, respiratory failure and ICU admission, though not statistically significant. Patients with hypertension, SLE and multi-comorbidities had a higher frequency of developing severe dengue, although not statistically significant. Severe dengue cases had a higher frequency of ICU admission. Of the 28 cases 9 (32.14%) patients died and 19 (67.86%) patients survived. (Figure 2)
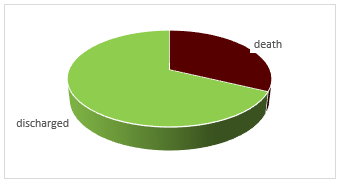
Figure 2: Final outcome of the study participants (n=28)
Patients who died had a significantly higher frequency of altered level of consciousness (4, 44.4% vs 0), and shock (8, 88.88% vs 1, 5.3%). There were no significant differences regarding abdominal pain, bleeding and pleural effusion between the survivors and non-survivors. (Figure 3)
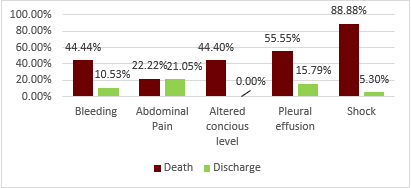
Figure 3: Comparative clinical features of dead and discharged patients (n=28)
Variables | Dead (n=9) | Discharged (n=19) | p-value |
TWBC Mean±SD | 13063.33±8072.51 | 4569.79±982.98 | 0.013a |
Lowest platelet count Median, IQR | 40000(19500—90500) | 75000 (51000—104000) | 0.142 |
Highest haematocrit Mean±SD | 36.04±4.72 | 35.28±5.31 | 0.715 |
Lowest haemoglobin Mean±SD | 9.12±1.44 | 9.51±2.32 | 0.65 |
Serum albumin Median, IQR | 23.7 (18.65—44.5) | 29 (29—30) | <0> |
ALT Median, IQR | 366 (174—1493.18) | 457.35 (72—457.35) | 0.629 |
AST Median, IQR | 267.5 (90.5—545) | 267.5 (80—267.5) | 0.468 |
Table 2: Laboratory parameters of the study participants (n=28)
TWBC= total white blood cell, SD=standard deviation, IQR=interquartile range, a=independent sample t-test, b=Mann-Whitney U-test
The total count of WBC was higher in non-survivor (p-value 0.013). Serum albumin was significantly lower in non-survivors. (Table 2)
| Univariate analyses | Multivariate analyses | ||||
Variables | Death (n=9) | Discharged (n=19) | p-value | aOR | 95% CI | p-value |
Male (n, %) | 4 (44.4) | 11 (57.9) | 0.689 |
|
|
|
Age (in years) Median, IQR | 38 (35—44) | 35 (28—55) | 0.562 |
|
|
|
DM | 3 (33.3) | 5 (26.3) | 1 |
|
|
|
HTN | 9 (100) | 16 (84.2) | 0.53 |
|
|
|
IHD | 0 | 3 (15.8) | 0.53 |
|
|
|
GN | 0 | 2 (10.5) | 1 |
|
|
|
Altered consciousness | 4 (44.4) | 0 | 0.006 |
|
|
|
Bleeding | 4 (44.4) | 2 (10.5) | 0.64 |
|
|
|
Shock | 8 (88.9) | 1 (5.3) | <0> | 144 | 7.97—2602 | 0.001 |
Pleural effusion | 5 (55.6) | 3 (15.8) | 0.068 |
|
|
|
WBC >12000/cmm | 5 (55.6) | 0 | 0.001 |
|
|
|
Platelet count <45000> | 6 (66.7) | 4 (21.1) | 0.035 |
|
|
|
Hypoalbuminaemia (<25> | 6 (66.7) | 1 (5.3) | 0.001 |
|
|
|
Hepatitis (ALT/AST>300 IU/L) | 7 (77.8) | 12 (63.2) | 0.67 |
|
|
|
Table 3: Risk factors of death in dengue-infected CKD patients on MHD (n=28) Univariate analyses Multivariate analyses
In the univariate model altered consciousness, shock, leukocytosis (>12000/cmm), thrombocytopenia (<45000>
Discussion:
This study investigated how ESRD patients with dengue presented at hospitals, what was their outcomes and what was the frequency of developing warning signs and severe dengue, and what laboratory parameters predicted mortality.
In our study, 57.2% of ESRD dialysis patients were between 20 and 39 years old, with a mean age of 41.18 ± 14.003 years. Similarly, a meta-analysis of 47 studies reported a significantly younger overall average age for dengue cases at 30.8 ± 14.5 years [6]. Interestingly, while previous studies by Chen et al., Kuo et al., and Rowe et al. highlighted older age (>65 years) as a risk factor for severe dengue, our findings show a different pattern, with a notable 57.2% of patients being in the younger age group [1,7,8].
In our study, 92.8% of CKD patients had hypertension, 32.14% had diabetes mellitus, 7.14% had glomerulonephritis, and 7.14% had ischemic heart disease. Similarly, Lee et al. found that 71.9% of their patients had hypertension, with 50% having diabetes [9]. Chen et al. also reported cardiovascular diseases (63.3%) and diabetes (53.1%) as the most common comorbidities in their study [1].
In the present study, the most common clinical features were fever (92.8%), loose motion (46.42%), shock (32.14%), bleeding (21.42%) altered conscious level (14.28%). Lee et al. also reported the three most common signs and symptoms were fever (76.6%), myalgia (26.6%), and altered consciousness (23.4%) [9].
In our study, 21 out of our 28 patients had WHO recommended warning signs. Common warning signs identified in ESRD dengue infected patients were breathlessness (35.71%), vomiting (32.14%), bleeding (21.42%), pleural effusion (21.42%), and abdominal pain (14.28%). Other research had similarly found vomiting to be a frequently reported symptom in dengue cases, with prevalence rates ranging from 36.1% to 55.9%, while abdominal pain has been noted in 32.1% to 52.9% of patients [1,10,11]. Brkovic et al. reported that abdominal pain occurs in 9.3% to 18% of cases, and Asgari et al. documented vomiting in 11.7% of patients [12,13]. These clinical features often mimic those of uremia, making diagnosis of warning signs more challenging. Moreover, important diagnostic markers such as hemoconcentration, pleural effusions, and hypoalbuminemia—critical for identifying Dengue hemorrhagic fever—may easily be overlooked when uremia is present [14]. Patients with multiple co-morbidities presentated with warning sign which were statistically significant. Warning signs at
presentation had more complications such as plasma leakage, severe dengue, respiratory failure and ICU admission. This emphasizes the critical role of early recognition and monitoring of warning signs in ESRD dengue patients to mitigate the risk of severe dengue-related complications.
Among the ESRD dialysis patients 32.14% was detected with severe dengue. This percentage is significantly higher compared to the general population, where the occurrence ranges from 4.7% to 16.5% [15,16,17].
Chen et al also reported that 36.7% of CKD patients in their study developed severe dengue [1]. The higher frequency may be due to complex pathophysiology related to ESRD. Due to Dengue, vessels become leaky causing plasma leakage and low blood pressure. According to WHO guidelines, the recommended fluid resuscitation for preventing severe dengue is not suitable for patients with ESRD, as their inability to produce urine (anuria) puts them at risk of developing volume overload and pulmonary edema. Also, this group of patients experience intradialytic hypotension as a result of decreased intravascular volume. Bleeding is one of the serious complications of dengue, which occurs due to thrombocytopenia and coagulation disorder. Patients with ESRD have an inherent risk of bleeding due to platelet dysfunction and the routine use of heparin during hemodialysis. [18,19,20].
In the present study, univariate analysis revealed significant differences in laboratory findings between patients who were discharged and those who died. However, multivariable analysis identified only an elevated white blood cell count at initial presentation (median: 7.3 × 10⁹ cells/L) as an independent predictor of poor outcomes. Although leukopenia (median: 4.0 × 10⁹ cells/L) is a common feature in dengue, with leukocyte counts typically reaching their lowest point between the 4th and 6th day after onset of symptoms, patients who died presented earlier (median: 3 days after symptom onset). During hospitalization, most of these patients developed leukocytosis (median: 13.9 × 10⁹ cells/L). Additionally, our study found that the majority of deceased patients were already in critical condition, such as presenting with shock, at the time of hospital admission. Therefore, prompt assessment and optimal supportive management are essential for these patients. Multivariate analysis identified leukocytosis, altered consciousness and pulmonary edema, as independent predictors of mortality among hospitalized ESRD patients with dengue infection. Additionally, Lee et al, revealed both severe hepatitis and leukocytosis and were independently associated with an increased risk of death within the first 7 days of illness onset.[9].
In our study, the mortality was 32%. Chen et al. reported an in-hospital mortality rate of 8.2% among ESRD patients, while Jabin et al. documented a rate of 20% [1,14] Furthermore, other research has indicated that patients with advanced renal dysfunction face an increased risk of mortality [21].
Limitations
This study has several limitations. First, the sample size was relatively small, which may limit the generalizability of the findings. Additionally, we did not conduct long-term follow-up after patient discharge, resulting in a lack of data on ongoing health outcomes and potential long-term effects. These limitations suggest that future studies should aim for larger sample sizes and implement comprehensive follow-up protocols to provide a more robust analysis of the outcomes over an extended period.
Conclusion
The study highlights the vital importance of early recognition of warning signs in ESRD dialysis patients to prevent severe complications related to dengue. The high mortality rate emphasizes the urgent need for targeted interventions and careful management strategies within this high-risk population.
References
- Chen HJ, Tang HJ, Lu CL, Chien CC. (2020). Warning signs and severe dengue in end stage renal disease dialysis patients. Journal of Microbiology, Immunology and Infection.;53(6):979-985.
View at Publisher | View at Google Scholar - Directorate General of Health Services (DGHS) of Bangladesh website
View at Publisher | View at Google Scholar - Chi C-Y, Sung T-C, Chang K, Chien Y-W, Hsu H-C, Tu Y-F, Huang Y-T and Shih H-I. (2023). Development and Utility of Practical Indicators of Critical Outcomes in Dengue Patients Presenting to Hospital: A Retrospective Cross-Sectional Study Tropical Medicine and Infectious Disease. 8 188
View at Publisher | View at Google Scholar - Lee K, Hsieh CJ, Lee CT, Liu JW. (2020). Diabetic patients suffering dengue are at risk for development of dengue shock syndrome/severe dengue: Emphasizing the impacts of co-existing comorbidity (ies) and glycemic control on dengue severity. Journal of Microbiology, Immunology and Infection.;53(1):69-78.
View at Publisher | View at Google Scholar - Ajlan BA, Alafif MM, Alawi MM, Akbar NA, Aldigs EK, Madani TA. (2019). Assessment of the new World Health Organization's dengue classification for predicting severity of illness and level of healthcare required. PLoS Neglected Tropical Disease. Aug 20;13(8): e0007144.
View at Publisher | View at Google Scholar - Badawi A, Velummailum R, Ryoo SG, Senthinathan A, Yaghoubi S, Vasileva D. (2018). Prevalence of chronic comorbidities in dengue fever and west nile virus: A systematic review and meta-analysis. PLoS One.;13: e0200200
View at Publisher | View at Google Scholar - Kuo HJ, Lee K, Liu JW. (2018). Analyses of clinical and laboratory characteristics of dengue adults at their hospital presentations based on the World Health Organization clinical-phase framework: Emphasizing risk of severe dengue in the elderly. Journal of Microbiology, Immunology and Infection.;51(6):740-748.
View at Publisher | View at Google Scholar - Rowe EK, Leo YS, Wong JGX, Thein TL, Gan VC, Lee LK. (2014). Challenges in Dengue Fever in the Elderly: Atypical Presentation and Risk of Severe Dengue and Hospita-Acquired Infection. PLoS Negl Trop Dis.;8: e2777.
View at Publisher | View at Google Scholar - Lee IK, Lee NY, Huang WC, Hsu JC, Tai CH, Yang CH, Huang CH, Lin CY, et.al. (2023). In-hospital mortality predictors among hospitalized adults and those with chronic kidney disease with dengue. J Microbiol Immunol Infect.;56(5):996-1006.
View at Publisher | View at Google Scholar - Tamibmaniam J, Hussin N, Cheah WK, Ng KS, Muninathan P. (2016). Proposal of a clinical decision tree algorithm using factors associated with severe dengue infection. PLoS One.; 11:1-10.
View at Publisher | View at Google Scholar - Ahmad MH, Ibrahim MI, Mohamed Z, Ismail N, Abdullah MA, Shueb RH. (2018). The sensitivity, specificity and accuracy of warning signs in predicting severe dengue, the severe dengue prevalence and its associated factors. Int J Environ Res Public Health.;15
View at Publisher | View at Google Scholar - Brkovic T, Burilovic E, Puljak L. (2016). Prevalence and severity of pain in adult end-stage renal disease patients on chronic intermittent hemodialysis: a systematic review. Patient Prefer Adherence.; 10:1131-1150 28.
View at Publisher | View at Google Scholar - Asgari MR, Asghari F, Ghods AA, Ghorbani R, Hoshmand MN, Rahaei F. (2016). Incidence and severity of nausea and vomiting in a group of maintenance hemodialysis patients. J Ren Inj Prev.; 6:49-55.
View at Publisher | View at Google Scholar - Jabin M, Mostafi M, Shahriar A, Alamgir S, Chowdhury T, Billah M. (2023). Dengue in End Stage Renal Disease Patients – A Case Series from a Tertiary Renal Centre of Bangladesh. J Bangladesh Coll Phys Surg.; 41: 92-95
View at Publisher | View at Google Scholar - Thein TL, Gan VC, Lye DC, Yung CF, Leo YS. (2013). Utilities and Limitations of the World Health Organization 2009 Warning Signs for Adult Dengue Severity. PLoS Negl Trop Dis.; 7:1-6.
View at Publisher | View at Google Scholar - Wanigasuriya K, Gurugama P, Wijewickrama A, Seneviratne SL, Gunatilake SB. (2011). Usefulness of WHO dengue case classifications in a Sri Lankan clinical setting Usefulness of World Health Organization (WHO) dengue case classifications in a Sri Lankan clinical setting. J Ceylon Coll Physicians.; 42:21-27.
View at Publisher | View at Google Scholar - Barniol J, Gaczkowski R, Barbato EV, da Cunha RV, Salgado D, Martínez E. (2011). Usefulness and applicability of the revised dengue case classification by disease: multi-centre study in 18 countries. BMC Infect Dis.; 11:106
View at Publisher | View at Google Scholar - Srikiatkhachorn A. (2011). Plasma leakage in dengue haemorrhagic fever. Thromb Haemost. 2009; 102:1042-1049.
View at Publisher | View at Google Scholar - Hottz E, Tolley ND, Zimmerman GA, Weyrich AS, Bozza FA. Platelets in dengue infection. Drug Discov Today Dis Mech.;8: e33-8.
View at Publisher | View at Google Scholar - Wills BA, Oragui EE, Stephens AC, Daramola OA, Dung NM, Loan HT. (2002). Coagulation Abnormalities in Dengue Hemorrhagic Fever: Serial Investigations in 167 Vietnamese Children with Dengue Shock Syndrome. Clin Infect Dis.; 35:277-285.
View at Publisher | View at Google Scholar - E de Francesco Daher, B Braz, et al. WCN23-1247 CKD Associated with increased mortality in dengue fever. Kidney International Reports, Volume 8, Issue 3, S39 - S40
View at Publisher | View at Google Scholar
