

Research Article | DOI: https://doi.org/10.31579/2834-5142/105
Comparison of Percutaneous and Laparoscopic Insertion of a Novel Three-Cuff PD Catheter: A Single-Center Study
- Mohamed Nasreldin 1*
- Abdullah Alhwiesh 1
- Muaz Abdelgalil 1
- Muthana Al Sahlawi 1
- Mariem Alkhaldi 1
- Hassan AlJassas 1
- Suzan Al Oudah 1
King Fahad Hospital of the University, Department of Nephrology, Saudi Arabia.
*Corresponding Author: Mohamed Nasreldin, King Fahad Hospital of the University, Department of Nephrology, Saudi Arabia.
Citation: Mohamed Nasreldin, Abdullah Alhwiesh, Muaz Abdelgalil, Muthana A. Sahlawi, Mariem Alkhaldi, Suzan Al Oudah, et al, (2025), Comparison of Percutaneous and Laparoscopic Insertion of a Novel Three-Cuff PD Catheter: A Single-Center Study, International Journal of Clinical Nephrology. 4(4); DOI:10.37579/2834-5142/105
Copyright: © 2025, Mohamed Nasreldin. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 June 2025 | Accepted: 30 June 2025 | Published: 05 August 2025
Keywords: achievement motivation; clean sport; doping; performance; enhancing substances
Abstract
A peritoneal dialysis catheter can be inserted using laparoscopic (basic or advanced), open surgical, or percutaneous techniques (with or without imaging guidance). Looking at the practice pattern worldwide, Open surgical dissection remains the most common insertion technique (8). The preferred procedure in the current literature is an advanced laparoscopic insertion if the patient has a history of major abdominal surgery or highly suspected intra-abdominal adhesions. This is due to the lowest risk of complications associated with this technique. Regardless of what surgical technique is used, the care of the peritoneal dialysis (PD) catheter after insertion is to make sure that adequate healing of the surgical wound and continued patency of the catheter for eventual initiation of regular peritoneal dialysis. The aim of this study was to look at the practice pattern and outcomes of the novel three-cuff PD catheter insertion at our center from 2015 to 2024.
Previous studies have reported significant variation in outcomes based on catheter insertion technique, and to date, no large randomized controlled trials (RCTs) have been performed to establish definitive superiority of one method over the other. The 2019 Japanese Society of Dialysis Therapy Peritoneal Dialysis Guidelines also confirm this lack of high-level evidence, emphasizing the importance of clinical context and expertise in selecting the appropriate technique.
Methods:
The cross-sectional study included 225 patients with end-stage kidney disease who had undergone PD catheter insertion, either percutaneous or laparoscopic in the nephrology unit at King Fahad Hospital University over nine years, from 2015 to 2024.
Results:
Our analysis showed that the relative risk of three-month complications was significantly higher in the percutaneous group, particularly involving catheter malfunction, leakage, and hernia. These findings are in line with previous literature supporting laparoscopic techniques for superior placement and reduced early complications. Figure 2 shows the positioning of the catheter after laparoscopic insertion.
There was no statistical significance between the two groups in terms of patient characteristics such as sample size, age, hypertension, diabetes mellitus, body mass index, and polycystic kidney disease. However, the study reported a higher prevalence of CHF, greater risk of technique failure, and increased complications at three months in the percutaneous PD catheter group compared to the laparoscopic group. However, the rate of catheter migration and peritonitis was 0% with the use of a three-cuff PD catheter.
Conclusion:
The availability of both methods and the use of the novel three-cuff PD catheter can help increase the number of patients who may benefit from peritoneal dialysis with the minimum possible complications post-insertion, particularly catheter migration and peritonitis, regardless of which surgical method is used.
Introduction
The main function of a peritoneal dialysis catheter is to allow consistent, bidirectional flow of dialysate without difficulties or discomfort. The catheter's function relies upon its design, implantation site, and the system configuration used to perform dialysis exchanges. Preoperative mapping of various landmarks on the patient's abdomen can be helpful to ensure optimal catheter placement (1). The catheter placement should not be over belt or pant lines and skin folds should be visible to the patient and suited to the patient's hand preference. The ISPD 2016 guidelines stated that preoperative mapping should be performed with the help of a stencil specific to the catheter or free hand and with the patient in the supine position. Patients with obesity or significant skin folds may benefit from parasternal or upper abdominal catheters, and skin marking should be performed while the patient is standing (6). Patients who undergo surgical placement of the PD catheter will need to undergo preoperative testing with anesthesiology to determine the type of anesthesia that would be suitable for the procedure. The PD catheters used most are double-cuffed; the subcutaneous segment can be straight or swan-necked, and the intraperitoneal segment can be straight or coiled-tipped. However, our center prefers to use the novel three-cuff catheter (7).
A peritoneal dialysis catheter can be inserted using laparoscopic (basic or advanced), open surgical, or percutaneous techniques (with or without imaging guidance).
Looking at the practice pattern worldwide, Open surgical dissection remains the most common insertion technique (8). However, in the United States, laparoscopic methods are the most common insertion technique. As an example, in 2018, 60 percent of catheters inserted in the United States were placed by laparoscopic, 30 percent by image-guided percutaneous, and 10 percent by open surgical techniques (9). One should understand that the choice between the various catheter insertion techniques largely depends upon local procedural expertise, availability of resources such as operating room, laparoscopy, and fluoroscopy, whether the patient can tolerate general anesthesia or not, and whether additional procedures such as hernia repair require to be performed at the time of catheter insertion or not (10). The preferred procedure in the current literature is an advanced laparoscopic insertion if the patient has a history of major abdominal surgery or highly suspected intra-abdominal adhesions. This is due to the lowest risk of complications associated with this technique. Patients with AKI who need urgent dialysis can have the catheter inserted using the image-guided percutaneous technique.
Laparoscopic techniques:
It is a minimally invasive approach that allows complete visualization of the peritoneal cavity for PD catheter insertion [28]. The basic laparoscopic insertion begins with gaining access to the peritoneal cavity in a variety of ways at the discretion of the operating surgeon. Once pneumoperitoneum is achieved, inspection of the abdomen allows for precise placement of the additional port(s) for peritoneal catheter insertion and advancement. It is useful to place the initial port remote from prior surgical incisions to reduce the risk of poor visualization or inadvertent bowel injury. The advanced laparoscopic technique combines the basic laparoscopic insertion technique with additional preemptive procedures to reduce the risk of mechanical complications [9]. Not all these procedures are required in every patient.
Percutaneous techniques:
Image-guided percutaneous (Seldinger) technique of catheter insertion is typically performed by radiologists or interventional nephrologists and is the second most common technique used in the United States as well as in Saudi Arabia, but it is not widely available in the latter.
Open surgical technique:
Remains the most common technique used for placing PD catheters worldwide because it is economical (relative to laparoscopic insertion), does not require special equipment, and can be performed under local anesthesia or conscious sedation.
For patients with a history of multiple abdominal surgeries, patients who are obese, or patients who require other simultaneous procedures such as hernia repair, it is suggested to use an advanced laparoscopic catheter placement rather than another technique (Grade 2C). For uncomplicated patients and those unable to tolerate general anesthesia, there are no true outcome differences among the individual techniques, and therefore, the choice should be based on local expertise. Open surgical insertion remains the most common technique used for placing PD catheters worldwide because it is economical (relative to laparoscopic insertion), does not require special equipment, and can be performed under local anesthesia or conscious sedation. Regardless of what surgical technique is used, the care of the peritoneal dialysis (PD) catheter after insertion is to make sure that adequate healing of the surgical wound and continued patency of the catheter for eventual initiation of regular peritoneal dialysis.
Aim of the study:
To look at the practice pattern and outcomes of the novel three-cuff PD catheter insertion at our center from 2015 to 2024. This may help to understand the factors that govern and dictate nephrology physicians to choose between surgical techniques and if one method is superior to the other in terms of post-surgical complications.
Methodology
Note: This study was conducted as a cross-sectional analysis based on a quasi- experimental design. Patients were not randomized; the choice of insertion technique was based on physician discretion and availability. This design reflects real-world practice but may introduce potential confounding factors.
The cross-sectional study included 225 patients with end-stage kidney disease who had undergone PD catheter insertion, either percutaneous or laparoscopic in the nephrology unit at King Fahad Hospital University over nine years, from 2015 to 2024 (table1). Patients with acute kidney injury who underwent peritoneal dialysis were excluded from the study. All data variables such as gender, age, BMI, underlying comorbidities, type of PD catheter insertion, and post-surgical complications (e.g., catheter malfunction, bleeding, peritonitis, and other complications) had been collected from the hospital registry, after approval from the hospital ethical committee (tables 2 and 3). The statistical analysis of data for the standard deviation, p values, prevalence, odd ratios, and correlation between independent and dependent variables was performed using the SPSS software. Patients' characteristics are shown in Table 1. We declare no conflicts of interests between the authors.
| Patients | Percutaneous PD | Laparoscopic PD | P value |
| Number 225 | 117 patients | 108 patients | 1.0 |
| Age mean | 48.7 | 40.6 | 0.25 |
| DM | 51 patients | 37 patients | 0.39 |
| BMI mean | 26 | 26.5 | 1.0 |
| Hypertension | 78 patients | 89 patients | 0.36 |
| CHF | 12 | 0 | 0.002 |
| ADPKD | 1 patient | 4 patients | 0.55 |
| 3-months complications | 15 patients | 5 patients | 0.05 |
A 2-cm paramedian incision is made 1 - 2 cm above the umbilicus, followed by blunt dissection of the subcutaneous tissue with an artery forceps until the fascia anterior to the rectus muscle is reached. The peritoneum is then punctured using a 16-gauge needle. A guidewire (straight, 120 cm long, and 2 mm thick) is inserted into the peritoneal cavity through the 16-gauge needle, The guidewire is then removed, and PD fluids are insufflated through this incision using the catheter transfer set for connection and a pressure pump, an average of 3 to 5 L of warmed PD solutions are infused in the peritoneal cavity.
A small incision (about 1 cm) is made at the lateral aspect of the rectus muscle in the suprapubic area through which the trocar with the pull-away sheath is introduced at an oblique angle. The peritoneum was then entered followed by removal of the trocar leaving the pull-away sheath in place. Dilatation of the oblique passage is performed by a small dilator followed by a larger one. The three-cuff PD catheter is introduced caudally and obliquely through the pull-away sheath over a 90-cm length stylet into the peritoneal cavity.
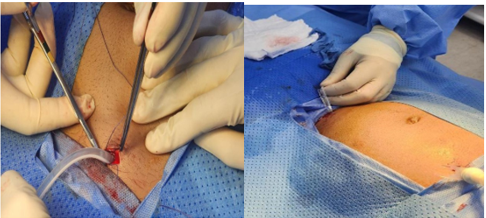
The PD catheter is advanced to a level that allows the external cuff to be in position at the anterior surface of the rectus muscle; the stylet is then removed, and the external cuff is secured with purse-string suture on the fascia anterior to the rectus muscle (Figure 1), a subcutaneous tunnel is then created obliquely lateral to the umbilicus using a stylet. The end of the catheter attached to the stylet is advanced into the tunnel and pulled out
The function of the catheter is checked by flushing PD solutions to rule out kinking or obstruction, and the position of the catheter tip inside the pelvis is confirmed by plain X-ray. The skin incisions are sutured.
Results
There was no statistical significance between the two groups in terms of patient characteristics such as sample size, age, hypertension, diabetes mellitus, body mass index, and polycystic kidney disease. However, there was statistical significance between the two groups, with more patients having chronic heart failure, diagnosed by echocardiography, in the percutaneous PD catheter group.
The prevalence of percutaneous PD catheter insertion practice among our studied population at King Fahad Teaching Hospital is that 52 % of our patients underwent percutaneous PD catheter insertion (table 2), compared to 48 % who underwent laparoscopic PD catheter insertion (table 3).
The prevalence of chronic heart failure among all patients in the cross-sectional study was 5.3% (12 out of 225 patients). All patients with heart failure underwent percutaneous PD catheter insertion, making the prevalence of CHF among this technique 0.102 (10%) compared to 0% among laparoscopic patients (table 2).
Percutaneous PD catheter insertions | Male | Female | Total |
Number | 55 | 62 | 117 |
Age (mean) | 53.9 | 43.5 | 48.7 |
Hypertension | 45 (81.8%) | 33 (53.2% | 78 |
DM | 30 (54.5%) | 21 (33.8%) | 51 |
BMI (mean) | 25.3 | 26.84 | 26 |
ADPKD | 0 | 1 (1.6%) | 1 (0.85%) |
CHF | 10 (18%) | 2 (3.2%) | 12 (10.2%) |
Post kidneytransplant | 0 | 0 | 0 |
Table 2
The overall prevalence of ADPKD among all patients was 0.022 (2.2%, 5 patients out of 225). The prevalence among laparoscopic patients was 0.037 (3.7%, 3 males and one female out of 108 patients), (table 3). Whereas the prevalence of ADPKD among percutaneous technique patients was 0.0085 (0.85%, one female patient out of 117), (table 2).
The incidence of failed first-time laparoscopic PD catheter insertion technique and use of percutaneous PD catheter insertion technique rather than repeating the laparoscopic technique was 0.009 (0.9%, only one male patient out of 108 patients), (table 4). The incidence of failed first-time percutaneous technique and the use of laparoscopic technique was 0.034 (3.4%, 3 males and one female out of 117 patients), (table 5). The relative risk of first-attempt failure in the percutaneous PD catheter insertion technique is 3.6 (elevated risk of technique failure), (table 5).
The prevalence of three-month complications in all patients who underwent either laparoscopic or percutaneous PD catheter insertion was 0.0977 (9.7%, 11 females and 10 males out of 225 patients), (table 4). However the prevalence of three-month complications was higher among the subcutaneous PD catheter group which was 0.128 (12.8%, 10 females and 5 males out of 117 patients), (table 5) compared to 0.046 (4.6%, 4 males and one female out of 108 patients) in the laparoscopic PD catheter group, (table 4).
The relative risk of post-PD catheter insertion three-month complications was 0.35, less than 1.0, which means that the risk of three-month complications may be reduced by the laparoscopic PD catheter insertion technique.
| Laparoscopic PD catheter insertions | Male | Female | Total |
| Number | 63 | 45 | 108 |
| Age(mean) | 39.7 | 41.5 | 40.6 |
| Hypertension | 48 (76%) | 41 (91%) | 89 (82.4%) |
| DM | 27 (42%) | 10 (22%) | 37 (34%) |
| BMI (mean) | 26.46 | 26.64 | 26.5 |
| ADPKD | 3 (4.7%) | 1 (2.2%) | 4 (3.7%) |
| CHF (mean) | 0 | 0 | 0 |
| Post kidney transplantation | 0 | 0 | 0 |
Table 3
Laparoscopic PD catheters | Male | Female |
First-time insertion (No. of patients) | 60 | 44 |
Insertion after a failed percutaneous technique (No. of patients) | 3 | 1 |
Three-month complications postlaparoscopic insertion | 4 (6.3%)due to hernia, leak, and omental wrap. Catheter migration 0 % Peritonitis 0% | 1 (2.2%)due to hernia Catheter migration 0% peritonitis 0% |
Table 4
Percutaneous PD catheter insertions | Male | Female |
First-time insertion (No. of patients) | 52 | 62 |
Insertion after a failed laparoscopic PD catheter insertion (No. of patients) | 1 | 0 |
Three-month complications postpercutaneous PD catheter insertions | 5 (one due to a leak and four needed catheter readjustments) | 10 (8 needed catheter readjustments, one developed a hernia, and one developed a leak. |
| Catheter migration 0% | Catheter migration 0% |
| Peritonitis 0% | Peritonitis 0% |
Table 5
Discussion
It is also worth emphasizing that this study uniquely used a novel three-cuff peritoneal dialysis catheter. Unlike the conventional two-cuff catheters reported in most prior studies, the three-cuff design used here completely eliminated catheter migration in both insertion groups. This suggests the catheter design itself may play a significant role in mitigating one of the most common early complications in PD.
This cross-sectional study compared patients' characteristics, clinical outcomes, and complications between two groups undergoing peritoneal dialysis catheter insertion: those who underwent percutaneous catheter placement and those who underwent laparoscopic placement. Our findings revealed a high prevalence of chronic heart failure (CHF) among patients in the percutaneous PD catheter group compared to the laparoscopic group. This disparity may be attributable to differences in patient selection, as patients with more comorbidities, such as CHF, may have been preferentially assigned to the percutaneous catheter insertion approach due to its less invasive nature. However, this observation highlights the need for further investigation to determine whether CHF independently influences outcomes following PD catheter insertion.
We also found a higher risk of technique failure in the percutaneous group due to catheter malfunction, mainly due to blood clots. This could be related to variations in catheter positioning when a blind technique is used and the formation of blood clots, which are resistant to alteplase catheter infusion. This finding is consistent with the current literature, prior studies have suggested that laparoscopic insertion offers better catheter placement and reduces the risk of post-insertion complications (8). Moreover, the relative risk of three-month complications was higher in the percutaneous group. These complications may include catheter malfunction, leaks, hernia, or mechanical issues, consistent with previous reports suggesting that laparoscopic placement provides superior visualization and allows for adjunctive procedures such as omentopexy to prevent complications. However, it is worth mentioning that the rate of the three-cuff PD catheter migration was 0 % and the rate of peritonitis in the first three months post-insertion was also 0%, this might be explained by the three-cuff PD catheter design, where only the small coiled functional segment of the catheter is present in the peritoneal cavity, which makes catheter migration impossible. Furthermore, the relatively long subcutaneous segment of the three-cuff catheter with the third cuff between the distal cuff and the exit site cuff may have contributed to the low rate of peritonitis in the first three months post- insertion. This observation underscores the potential benefits of laparoscopic approaches in patients who are at higher risk of technical challenges or early catheter- related issues. Interestingly, BMI was comparable between the two groups, indicating that differences in selection and outcomes were not influenced by body habits. This suggests that other factors such as catheter insertion technique, catheter type and design, underlying comorbidities, or perioperative management, may play a more prominent role in determining clinical success and complications rate.
As noted in prior reports and emphasized by the 2019 Japanese Society of Dialysis Therapy Guidelines, variation in technique outcomes may be influenced by operator experience and patient selection, further complicating direct comparisons in non-randomized studies.
Strengths and limitations:
The strengths of this study include a well-defined patient cohort and a direct comparison between two widely used PD catheter insertion techniques. However, the study was limited to its cross-sectional design, which precludes establishing causality. Additionally, the unique distribution of comorbidities, such as CHF, between the groups may have contributed to outcome differences. Future prospective randomized studies are warranted to validate our findings and explore strategies to optimize outcomes for patients undergoing PD catheter insertion.
Conclusion
This cross-sectional study highlights a higher prevalence of CHF, greater risk of technique failure, and increased complications at three months in the percutaneous PD catheter group compared to the laparoscopic group. However, the rate of catheter migration and peritonitis was 0% with the use of a three-cuff PD catheter. These findings emphasize the importance of careful patient selection and consideration of insertion techniques and PD catheter types, particularly in patients with significant comorbidities. The availability of both methods and the use of the novel three-cuff PD catheter can help increase the number of patients who may benefit from peritoneal dialysis with the minimum possible complications post-insertion, particularly catheter migration and peritonitis, regardless of which surgical method is used.
References
- Santarelli S, Amici G, Bernacconi T, et al. (2013). The peritoneal dialysis catheter J Nephrol.;26(Suppl 21):4–75
View at Publisher | View at Google Scholar - Di Paolo N, Petrini G, Garosi G, Buoncristiani U, Brardi S, Monaci G. (1996). A new self- locating peritoneal catheter Perit Dial Int.; 16:623–627
View at Publisher | View at Google Scholar - Bergamin B, Senn O, Corsenca A, et al. (2010). Finding the right position: A three-year, singlecenter experience with the “self-locating” catheter Perit Dial Int.;30:519–523
View at Publisher | View at Google Scholar - Moon JY, Song S, Jung KH, et al. (2008). Fluoroscopically guided peritoneal dialysis catheter placement: Long-term results from a single center Perit Dial Int.; 28:163–169
View at Publisher | View at Google Scholar - 5-Li PK, Szeto CC, Piraino B, de Arteaga J, Fan S, Figueiredo AE, Fish DN, Goffin E, Kim YL, et.al. (2016). ISPD Peritonitis Recommendations: 2016 Update on Prevention and Treatment. Perit Dial Int. Sep 10;36(5):481-508.
View at Publisher | View at Google Scholar - Sayer M, Thiel C, Schenk M, Königsrainer A, Heyne N, Birkenfeld AL, et.al. (2022). Intraperitoneal extension of the peritoneal dialysis catheter-a new technique for catheter implantation in patients with obesity. J Nephrol. Jan;35(1):311-316.
View at Publisher | View at Google Scholar - Hwiesh AKAI, Rahman ISA, Audah NAI, et al. (2017). A Novel three cuff peritoneal dialysis catheter with low entry technique: three years single center experience. Urol Nephrol Open Access J.;4(5):150-156.
View at Publisher | View at Google Scholar - Briggs VR, Jacques RM, Fotheringham J, Maheswaran R, Campbell M, Wilkie ME. (2023). Catheter insertion techniques for improving catheter function and clinical outcomes in peritoneal dialysis patients. Cochrane Database Syst Rev. Feb 22;2(2):CD012478.
View at Publisher | View at Google Scholar - Zheng S, Drasin T, Dybbro P, Darbinian JA, Armstrong MA, Bhalla NM. (2023). Advanced Image-Guided Percutaneous Technique Versus Advanced Laparoscopic Surgical Technique for Peritoneal Dialysis Catheter Placement. Kidney Med. Oct 31;6(1):100744.
View at Publisher | View at Google Scholar - Sodo M, Bracale U, Argentino G, Merola G, Russo R, Sannino G, Strazzullo T, Russo D. (2016). Simultaneous abdominal wall defect repair and Tenckhoff catheter placement in candidates for peritoneal dialysis. J Nephrol. Oct;29(5):699-702
View at Publisher | View at Google Scholar - (2019). Japanese Society for Dialysis Therapy. Guidelines for Peritoneal Dialysis. Tokyo: Japanese Society for Dialysis Therapy.
View at Publisher | View at Google Scholar
