

Research Article | DOI: https://doi.org/10.31579/2835-2882/103
Comparison and Calculation of Absorbed Dose Rate in the Bone Marrow by the Mammosite and Contura Applicators in Breast Cancer Brachytherapy with Mcnp Simulation
1School of Advanced Technologies in Medicine, Tehran University of Medical Sciences, Tehran, Iran.
2Physics and Medical Engineering, Tehran University of Medical Sciences, Tehran, Iran.
*Corresponding Author: Fatemeh Mahdavi, School of Advanced Technologies in Medicine, Tehran University of Medical Sciences, Tehran, Iran.
Citation: Fatemeh Mahdavi, Hosseini Dokht AS, (2026), Comparison and Calculation of Absorbed Dose Rate in the Bone Marrow by the Mammosite and Contura Applicators in Breast Cancer Brachytherapy with Mcnp Simulation, Clinical Research and Studies, 5(1); DOI:10.31579/2835-2882/103
Copyright: ©2026, Fatemeh Mahdavi. this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 December 2025 | Accepted: 15 December 2025 | Published: 02 January 2026
Keywords: brachytherapy; mammosite applicator; contura applicator; breast; red bone marrow
Abstract
Introduction: Breast cancer is the most common cancer among women. With the increasing prevalence of this disease, the focus has been on new methods. Brachytherapy is one of the ways to treat breast cancer. This is a type of radiation therapy that is performed by providing a dose using radioactive sources located at the treatment site, therefore it is a good way to treat tumors.
Materials and methods: MCNP Code: The MCNPX code is one of the most powerful computational codes based on the Monte Carlo method. ORNL-MIRD Phantom: To calculate the dose, a model of the human body is required as a phantom. The analytical model of the human body is described by ORNL-MIRD publications. Mammosite applicator: Which is a tool for high-dose rate brachytherapy (HDR) and includes a duct for transmitting radioactive source, an elastic balloon, and a radioactive source. Mammosite-ML or Contura applicator: is almost identical to Mammosite, The difference is that the Mammosite has a central duct but the Mammosite-ML model has 3, 4 or 5 additional ducts around the central duct.
Result: Absorption dose rate of body organs by Mammosite applicator with target volume in the right breast: Target Volume: 7/01 × 10-1 , Left breast: 6/89 × 10-3, Right breast: 7/26× 10-1 ,Red bone marrow: 2/30 × 10-3 . Absorption dose rate of body organs by MammoSite applicator with target volume in the left breast: Target Volume: 7/02 × 10-1, Left breast: 7/26 × 10-1, Right breast: 6/88× 10-3, Red bone marrow: 2/27 × 10-3. Absorption dose rate of body organs by Contura applicator with target volume in the right breast: Target Volume: 9/77 × 10-1, Left breast: 1/04 × 10-2, Right breast: 6/8× 10-1, Red bone marrow: 2/06 × 10-3. Absorption dose rate of body organs by Contura applicator with target volume in the left breast: Target Volume: 9/74 × 10-1, Left breast: 6/6 × 10-1, Right breast: 1/06× 10-2, Red bone marrow: 2/03 ×10-3.
Conclusion: The absorbed dose by the bone marrow in the Contura applicator is reduced compared to the Mammosite applicator. This is due to the asymmetric dose distribution by the Contura applicator and the increase in the number of lateral ducts around the central duct.
Introduction
Breast cancer is the most common cancer among women. With the increasing prevalence of this disease, the focus has been on new methods. Brachytherapy is one of the ways to treat breast cancer. This is a type of radiation therapy that is performed by providing a dose using radioactive sources located at the treatment site, therefore it is a good way to treat tumors. Brachytherapy has the potential to be applied to most tumors and can be used as an initial treatment or combination therapy with external radiation therapy. The main advantage of brachytherapy is that the highest dose of radiation around the radioactive source is in the tumor site and with increasing distance from the radioactive source, the dose decreases sharply and the risk of exposure to adjacent healthy tissues (OAR: organ at risk) reduces the treatment site (tumor). In brachytherapy treatment systems, high-dose sources are used in tissues placement.
The Iridium-192 source, for the first time in 1976, was used at the University of Oxford for Brachytherapy and so far, there is a lot of use in this regard. The source of iridium-192 is a rare earth element. Iridium-192 is the Iridium-191 isotope, Iridium-192 is produced by the neutron activation of Iridium -191. It has a half-life of 73/8 days and decays by beta minus emission. [1]
This source is a capsule of platinum with an inner and outer diameter of 0.0325 and 0.045 cm respectively. This source emits beta beam with a 672 Kev energy and gamma rays with energies ranging from 136 kV to 1060 kV. The activity of the used source is 10 curies. The simulated source here is a cylinder with a length of 0.5 and a radius of 0.017 cm.
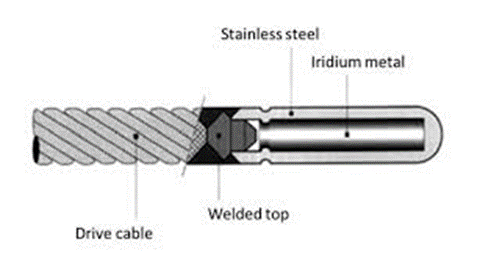
Figure 1: Iridium-192
In the past, these radioactive seeds were placed manually in place. This is called the manual interstitial implants method. This method has many disadvantages, including: the complexity of planting, the need for general anesthesia, the exposure of workers to radiation, and the inability to implement the principles of radiation protection, temporary or permanent
deformation of the breast tissue, breeding toxicity, ipsilateral breast failure (IBF), Severe pain and limitation of appointment in the presence of radioactive seeds at the site of treatment and impaired movement of the arms and hands. In response to these disadvantages, breast applicator was introduced.

Figure 2: Interstitial multi catheter breast brachytherapy
Materials and Methods:
MCNP Code: The MCNPX code is one of the most powerful computational codes based on the Monte Carlo method. To use this code, an input file with a specific structure of the problem information including geometry, material, source, output type, etc. should be provided. The code, with the input file information and the cross-section library, solves the problem and produces results in an output file.
ORNL-MIRD Phantom: To calculate the dose, a model of the human body is required as a phantom. The analytical model of the human body is described by ORNL-MIRD publications. All organs of the human body are represented by different geometries with analytic equations and due to the difference in the gender of the anatomy, it is presented in two male and female models. Of course, the child model is also available. In fact, the MIRD phantom provides an analytical model of the human body. Calculating doses in the organs requires a detailed description of the organ's geometry and chemical structure of the tissue.
Using this standard phantom, the absorbing dose and the equivalent dosage in different organs of the body and hence the effective dose of the patient are also calculated. In addition to geometric shapes, the chemical structure and density of specific body tissues are needed for absorbing dose calculations. All of these factors have been applied to the phantom. In this study, the female ORNL-MIRD phantom was used.
Figure 3: ORNL-MIRD phantom female model in facade XZ
Mammosite applicator: Mammosite Which is a tool for high-dose rate brachytherapy (HDR) and includes a duct for transmitting radioactive source, an elastic balloon, and a radioactive source. The radioactive source commonly used in this tool is Iridium-192 and the activity of the source is 10 curie.

Figure 4: Mammosite applicator
This device has a catheter that can be attached to the after loading machine (HDR Afterloader) connect to the source. The end of catheter is surrounded by a balloon that can be filled with salt or saline solution, water or other materials. The balloon is placed in the lumpectomy cavity. That's about 34 Gy can be treated twice a day between 5 to 10 minutes (every 1 to 5 minutes) in the 5 to 10 days. That is, in each session 3/4 Gy dosage for beneficial treatment should be absorbed into the target cell. The most common size of this balloon is 4-5 cm and 5-6 cm which has a volume between 34-113 cubic centimeters. The advantage of this device is its ease of use. [1]
With the modeling, put the applicator on both the right and left of the breast and a target volume or hypothetical tumor is placed within 1 cm of the applicator. The absorbed dose is calculated by the target cell, the treated breast, and red bone marrow.
Mammosite-ML or Contura applicator: Mammosite-ML is almost identical to Mammosite, The difference is that the Mammosite has a central duct but the Mammosite-ML model has 3, 4 or 5 additional ducts around the central duct. In this research, the applicator model with 5 additional ducts is also known, which is also known as the Contura Applicator. [1]
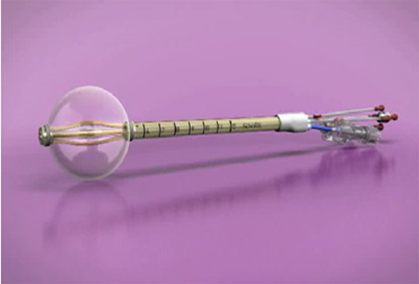
Figure 5: Mammosite-ML or Contura applicator
Knowing the exact distribution of doses by this source is very important in order to design a treatment method. In this project, two commonly used breast cancer treatment applicators called Mammosite and Mammosite-ML
or (Contura) are modeled by the Monte Carlo simulation code. Put the applicator on both the right and the left breast, and a target volume or hypothetical tumor is placed within 1 cm of the applicator. The absorbed dose is calculated by the target cell, the treated breast and red bone, which are the main target of the project and the absorbed dose rate in the tumor is monitored by the absorbed dose by the healthy tissue of the breast.
Result:
As stated above, the dose rate of high-dose brachytherapy (HDR) is on average 34 Gy to the tumor in 10 sessions of treatment. That is, in each session 3/4 Gy dosage for beneficial treatment should be absorbed into the target cell.
Simulation results of Mammosite applicator with target volume in right breast and absorption dose rate of body organs by Mammosite applicator with target volume in the right breast: Target Volume: 7/01 × 10-1, Left breast: 6/89 × 10-3, Right breast: 7/26× 10-1, Red bone marrow: 2/30 × 10-3.
Simulation results of Mammosite applicator with target volume in left breast and absorption dose rate of body organs by Mammosite applicator with target volume in the left breast:
Target Volume: 7/02 × 10-1, Left breast: 7/26 × 10-1, Right breast: 6/88× 10-3, Red bone marrow: 2/27 × 10-3.
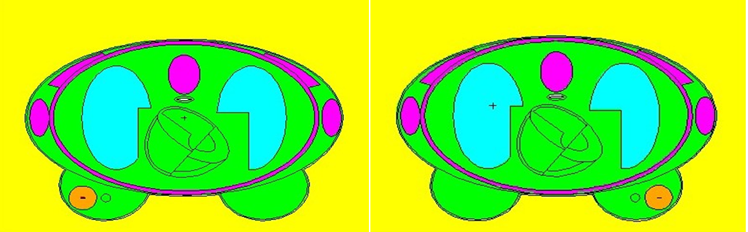
Figure 6: Mammosite applicator in right and left breast and a sphere with a distance of 1 cm in XY view
Simulation results of Mammosite-ML (Contura) applicator with target volume in right breast and absorption dose rate of body organs by Contura applicator with target volume in the right breast:
Target Volume: 9/77 × 10-1, Left breast: 1/04 × 10-2, Right breast: 6/8× 10-1, Red bone marrow: 2/06 × 10-3.
Simulation results of Mammosite-ML (Contura) applicator with target volume in left breast and absorption dose rate of body organs by Contura applicator with target volume in the left breast:
Target Volume: 9/74 × 10-1, Left breast: 6/6 × 10-1, Right breast: 1/06× 10-2, Red bone marrow: 2/03 ×10-3.
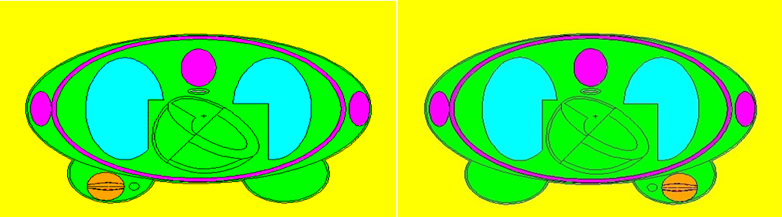
Figure 7: Mammosite-ML applicator in right and left breast and a sphere with a distance of 1cm in XY view
In the Mammosite applicator, the amount of absorbed dose in the treated breast is more than the hypothetical tumor or target volume and then the dose rate in the target volume is the highest, this could be a weak point for this applicator because the goal is to achieve the highest dose to the target volume, not other areas and healthy tissues of the breast.
In the contura applicator, the amount of absorbed dose before each organ is greater than the target volume or hypothetical tumor. In fact, the weakness of Mammosite, which has the highest doses, is absorbed by the breast, is not available in this applicator. Therefore, there is another reason to prove that treatment is better and less risky with this method (Contura applicator). After the target volume, the treated breast tissue has the target volume received a significant dose.
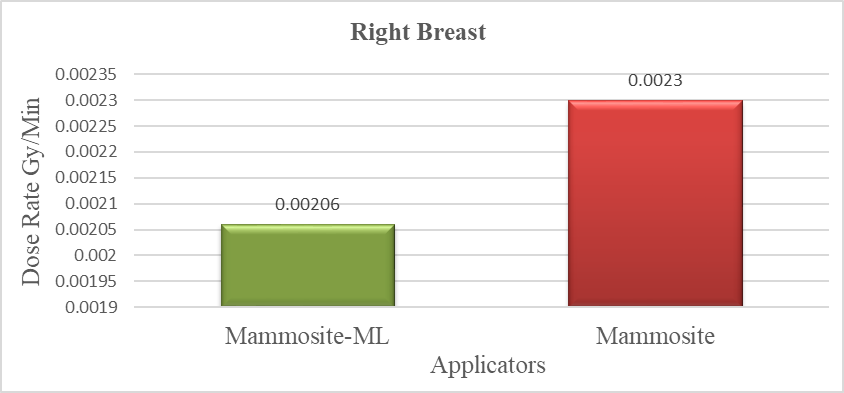
Chart 1: Bone marrow absorption dose chart by Mammosite and Contura applicators when the right breast is treated

Chart 2: Bone marrow absorption dose chart by Mammosite and Cantura applicators when the left breast is treated
According to the results, the Mammosite applicator was unable to distribute asymmetric doses. But the contura applicator is promising asymmetric dose distribution and higher quality treatment and it can create a safer and better quality treatment. Therefore, the research hypothesis suggests that by increasing the number of channels, the ability to produce asymmetric doses increases and the treatment will be better, it's true.
In the contura applicator, according to the absorption dose ratio of the right and left breast tissue to the absorbed dose by the target volume, the number is 0.69 and 0.67 respectively. Which indicates a low proportion, so it can be concluded that the same dosage, that reached the tumor tissue did not affect the amount of doses to the healthy tissue of the breasts. This represents an asymmetric dose and proves that the contura applicator is capable of asymmetric distribution. Calculations and hypothesis of the project are quite correct.
The accuracy of the project is calculated by considering the ability of the Monte Carlo code to estimate the error rate by the software itself, which is almost equal to 5%, that's an acceptable number. On the other hand, the numbers obtained from the absorbed dose in both simulated applicators were quite logical according to the body's anatomy. The absorption dose rate in both applicators did not differ from the target volume in the right breast or when the target volume was in the left breast.
Conclusion:
The absorbed dose by the bone marrow in the Contura applicator is reduced compared to the Mammosite applicator. This is due to the asymmetric dose distribution by the Contura applicator and the increase in the number of lateral ducts around the central duct. According to the principles of radiobiology and radiation protection, it is proven that after white blood cells, bone marrow has the highest sensitivity and can reduce hypoplasia if the absorbed dose is between (200-1000) rad or (2-10) Gy.
Therefore, the lower the absorbed dose by the bone marrow, the lower the complications and the potential risks.These results suggest Contura applicator capable of asymmetric dose distribution should be used for breast brachytherapy.
References
- Peter Hoskin, DR Catherine Coyle, (2011). Radiotherapy in Practice Brachytherapy, Second Edition, Oxford University.
View at Publisher | View at Google Scholar - David J, Brenner, (1997).DSc Center for Radiological Research, College of Physicians and Surgeons, Columbia University, New York Radiation Biology in Brachytherapy Journal of Surgical Oncology, 65:66–70.
View at Publisher | View at Google Scholar - Eric Alan Williams, (2012). Dose modification factor analysis of multi-lumen brachytherapy applicator with Monte Carlo simulation, The University of Toledo.
View at Publisher | View at Google Scholar - Christopher F Njeh, Mark W Saunders, Christian M Langton, (2010).Accelerated Partial Breast Irradiation (APBI): A review of available techniques, Radiation Oncology Journal.
View at Publisher | View at Google Scholar - Breast brachytherapy (using multicatheters) using ultrasound in Radiation Oncology, Health Facts, University of Wisconsin Hospitals and Clinics Authority,
View at Publisher | View at Google Scholar - Daniel Scanderbeg, Catheryn Yashar, (2010).Greg White, Roge Rice, Tod Pawlicki, Evaluation of three APBI techniques under NSABP P-39 guidelines, Journal of applied Clinical Medical Physics,Department of Radiation Oncology,UC, San Diego CA, USA, Winter.
View at Publisher | View at Google Scholar - Craig Koontz, (2013). Monte Carlo Investigation on the Effect of Heterogeneities on Strut Adjusted Volume Implant (SAVI) Dosimetry Thesis, The University of Toledo.
View at Publisher | View at Google Scholar - Yongbok Kim, Mark G.Trombetta, (2014). Dosimetric evaluation of multilumen intracavitary balloon applicator rotation in high-dose-rate brachytherapy for breast cancer, Journal of applied clinical medical physics.
View at Publisher | View at Google Scholar - Joseph F, Harmon Jr, Brandon K. Rice, (2013). Comparison of planning techniques when air/fluid is present using the strut-adjusted volume implant (SAVI) for HDR-based accelerated partial breast irradiation, Department of Radiation Oncology, Bon Secours Cancer Institute, Henrico, VA, USA.
View at Publisher | View at Google Scholar - Breast brachytherapy (using multicatheters) using ultrasound in Radiation Oncology, Health Facts, University of Wisconsin Hospitals and Clinics Authority, 2014.
View at Publisher | View at Google Scholar - Daniel Scanderbeg, Catheryn Yashar, Greg White, Roge Rice, Tod Pawlicki, Evaluation of three APBI techniques under NSABP P-39 guidelines, Journal of applied Clinical Medical Physics, Department of Radiation Oncology,UC, San Diego CA, USA, Winter 2010.
View at Publisher | View at Google Scholar - Vicini F, Jaffray D, Horwitz E et al. (1998). Implementation of 3D-virtual brachytherapy in the management of breast cancer: a description of a new method of interstitial brachytherapy. International Journal of Radiation Oncology Biology Physics 40:62935.
View at Publisher | View at Google Scholar - Vicini F,Beitsch P,Quiet C,Gittleman M,Zannis V,Fine R et al.(2011).Five-year analysis of treatment efficacy and cosmesis by the American Society of Breast Surgeons Mammosite Breast Brachytherapy Registry Trial in patients treated with accelerated partial breast irradiation.International Journal of Radiation Oncology Biology Physics.
View at Publisher | View at Google Scholar - (2014).Breast brachytherapy (using multicatheters) using ultrasound in Radiation Oncology, Health Facts, University of Wisconsin Hospitals and Clinics Authority.
View at Publisher | View at Google Scholar
