

Case Report | DOI: https://doi.org/10.31579/2835-9259/004
Case Report: Neurological Complications of Thread Lifting
1 Candidate of Medical Sciences, board-certified physician, plastic surgeon, cosmetologist, Junior Research Assistant at the A.I. Burnazyan Federal Medical Biophysical Center of the FMBA of Russia, member of the Interregional Public Organization for Botulinum Therapy and Russian Society of Plastic, Reconstructive and Aesthetic Surgery.
2 Candidate of Medical Sciences, neurologist at the Central Institute of Botulinum Therapy and State-of-Art Neurology, member of the Interregional Public Organization for Botulinum Therapy.
*Corresponding Author: Ivan Ivanovich Gribanov, Ivan Ivanovich Gribanov. Candidate of Medical Sciences, board-certified physician, plastic surgeon, cosmetologist, Junior Research Assistant at the A.I. Burnazyan Federal Medical Biophysical Center of the FMBA of Russia, member of
Citation: II Gribanov and Konovalova Z.N, (2022) Case Report: Neurological Complications of Thread Lifting. Oral Health and Dentistry Case Reports.1(1); DOI:10.31579/2835-9259/004
Copyright: © 2022 Ivan Ivanovich Gribanov, This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 October 2022 | Accepted: 19 October 2022 | Published: 31 October 2022
Keywords: thread lifting; complications; neuropathy
Abstract
State-of-art invasive cosmetic procedures in some cases can lead to the development of neurological complications, in particular neuropathy. Neuropathy can be manifested by sensory (pain), motor and autonomic disorders. Neurological complications of thread lifting are associated with injury to both sensory and motor nerves; facial and trigeminal nerves are most commonly affected. In case of direct nerve injury with a needle, cannula or thread, acute neuropathy occurs. Compression nerve injury is associated with a delayed symptoms development. Clinical signs of sensory nerve injury may include paresthesia, dysesthesia, anesthesia, and neuropraxia.
Nerve endings completely restore within up to 6 months, but in some cases, the injury can be catastrophic. The article presents the authors’ personal clinical observations.
Introduction
The increase in the number of invasive procedures in cosmetology has led to an increase in the number of various complications, which is associated with both high traumatism of the new methods and insufficient qualification of a specialist, as well as non-compliance with post-procedural protocols, anatomical features, as well as concomitant diseases (SV Surovykh, OR Orlova, AI Nerobeev et al. Facial nerve injury in plastic surgery. Annals of Plastic, Reconstructive and Aesthetic Surgery, 2011;(1):8–30.; ZN Konovalova ‘Botulinum therapy in neuropathic disorders in cosmetology’ Aesthetic Medicine Vol. XIX • No. 3 • 2020
Metamorphoses No. 30/31; September, 2020. Thread techniques for correction of the age-related facial changes can be divided into two large groups. The first is the use of threads of various sizes and configurations for the reinforcement of the skin or the so–called ‘mesothreads’. The second is the use of threads with various types of offsets, notches with fixation to connective tissue structures — the so-called lifting threads. Both techniques are associated with the risk of undesirable effects and complications characteristic of invasive methods — pain, hematomas, inflammation. Neurological complications (neuropathies) are particularly challenging.
Neuropathy is a disease of the peripheral nervous system characterized by an injury to the peripheral nerve fibers that make up various nerves. Neuropathy can be manifested by sensory (pain), motor and autonomic disorders. [DR Shtulman, OS Levin. Neurology: practitioner’s handbook.-M.: MEDpress-inform, 2008.]. Signs of nerve injury may vary in severity. In case of direct nerve injury with a needle, cannula or thread, acute neuropathy occurs. Compression nerve injury is associated with a delayed symptoms development.
Neurological complications of thread lifting are associated with an injury to both sensory and motor nerves. Facial and trigeminal nerves are most often affected, which is shown in the figure with indication of the most common directions of application of the lifting threads. (Fig. 1) [SV Surovykh, OR Orlova, AI Nerobeev et al.
Facial nerve injury in plastic surgery. Annals of plastic, reconstructive and aesthetic surgery, 2011;(1):8–30.]
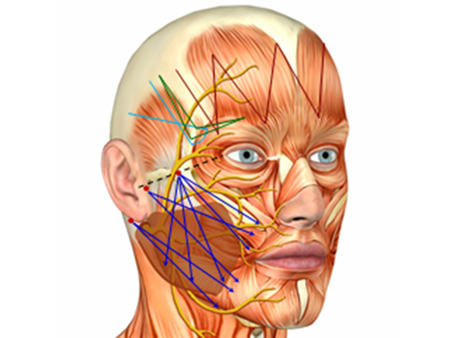
Figure 1. The most common thread application patterns.
An injury to the structures of motor nerves causes partial or complete paralysis of the corresponding muscles. (OR Orlova, YuV Mozolevsky, LR Mingazova. Facial neuropathy (Bell’s palsy). In: Selected lectures on Neurology II. — M.: MEDpressinform, 2012:381–394.) The most serious are injuries to the facial nerve branches, since they cause paresis or plegia of the facial muscles, facial asymmetry and serious functional and aesthetic defects.
In some cases, the facial nerve injury is so serious that it can be considered serious harm to the health and may lead to criminal liability of the doctor. (Order of the Ministry of Healthcare and Social Development of the Russian Federation No. 194n dated 24 April 2008. — https://www.rosminzdrav.ru) Injuries to the frontal, buccal, zygomatic and the marginal mandibular branches of the facial nerve are most common. (K Watanabe, et al. Anatomy for Plastic Surgery of the Face, Head, and Neck, by Thieme Medical Publishers, Inc., 2016, p. 241) In cases of an injury to the temporal branch of the facial nerve, the consequences may be permanent, since the frontal muscle does not have additional innervation. (AV Triumfov. Topical diagnostics of diseases of the nervous system. — M.: MEDpress, 1998. — p. 342
MG Prives, NK Lysenkov, VI Bushkovich. Human anatomy. — M.: Medicine, 1985. — 672 p.) Thread lifting is most often performed in the buccal-zygomatic area and injuries to the zygomatic and buccal branches of the facial nerve are most common. (S Standring et al. Gray’s Anatomy. The Anatomical Basis of Clinical Practice, 2016, 41th ed. Elsevier Limited, с. 2252.
MG Prives, NK Lysenkov, VI Bushkovich. Human anatomy. — M.: Medicine, 1985. — 672 p.) The most dangerous anatomical area of the skin is limited by a triangle with the apex located on the zygomatic buttress and connected to the angle of mouth and the mandibular angle. During manipulations on the lower third of the face, there is a risk of an injury to the marginal mandibular branch, which innervates the depressor muscle of the angle of the mouth, depressor muscle of lower lip and mental muscle (Fig. 2) [3]. Alessio Redaelli. Dangerous areas of the face, how to avoid complications: simple rules for safe aesthetic correction, 2018, [3].
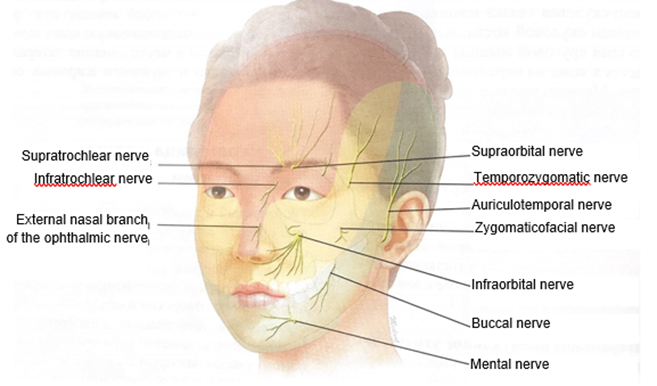
Figure 2. Facial nerve branches exit points.
Signs of an injury to the branches of the sensitive trigeminal nerve include impaired sensation and pain of various severity. (LINK. LR Mingazova, EI Karpova, OR Orlova. Neuropathic disorders in the facial area after contouring injections // Injection procedures in cosmetology. - 2010.- No. 2.- pp. 2-8
ZN Konovalova ‘Botulinum therapy in neuropathic disorders in cosmetology’ Aesthetic Medicine Vol. XIX • No. 3 • 2020
Metamorphoses No. 30/31; September, 2020)
Thus, sensory nerve injuries manifest in the following forms:
- paresthesia — tingling, pain or burning, may occur as an early or delayed signs of nerve injury.
- dysesthesia is an abnormal sensation of pain, itching, burning or other discomfort that occurs spontaneously or after stimulation, often develop as a late sign of sensory nerve injury.
- anesthesia — numbness over the skin area; often it is an early and immediate result of nerve injury.
Resolution of changes after the sensory nerve injuries usually occurs completely due to a sufficient number of sensory nerves over a period from several weeks to 6 months, but in some cases, complications can be catastrophic. A combination of motor and sensory disorders is also possible.
Anatomically, there are 8 dangerous areas associated with the invasive procedures (Fig. 3) [1]:
- Supraorbital and supratrochlear branches of the ophthalmic branch of the trigeminal nerve and the corresponding vessels.
- The infraorbital trunk of the maxillary branch of the trigeminal nerve and the infraorbital vessels.
- Mental nerve and blood vessels (injuries occur rarely, as they lie on the surface of the bone).
- Temporal part of the facial nerve.
- The marginal mandibular branch of the facial nerve and the corresponding branch of the facial artery.
- Buccal and zygomatic nerves and the Stenon duct of the parotid gland.
- Posterior triangle of neck.
- The area has an inverted conical shape, it is located anteriorly to the ear, bounded by the auricle and the mandibular branch posteriorly, mandibular branch inferiorly, the masticatory muscles anteriorly and the tragus superiorly.
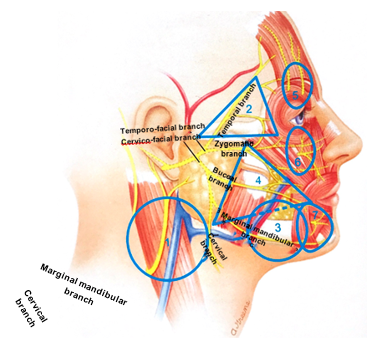
Figure 3. Dangerous areas of the face.
The most common causes of injury to the nerve endings during thread lifting are violations of the technique of thread application with non-compliance with the depth of implantation.
In addition, various specific anatomical features of the facial structures are possible — deficiency of subcutaneous fat and superficial course of nerve trunks.
1. Threads parameters play an important role, since exceeding the permissible thickness of the threads increases the risk of injury to the nerve trunks (Fig. 4)
2. Thread thickness (maximum permissible thickness of lifting threads is 1-0 (0) USP, d = 0.4 mm). Thread thickness can be measured in the European metric or United States customary units (USP) systems. Both standards are used in Russia, the ratio between them is as follows:
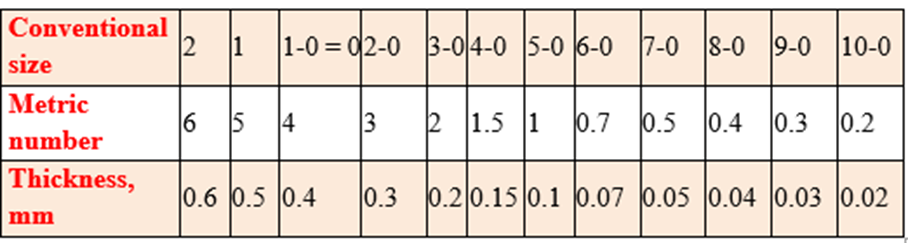
Figure 4. Maximum allowable thread thickness.
Treatment tactics in case of injury in compliance with the protocol includes the following:
- Glucocorticosteroids for rapid relieve of swelling — IV drip — dexamethasone (4–8 mg IV).
- Antiedemic procedures (magnetotherapy, UHF, lymphatic drainage, HBO).
- Berlithion 600 mg OD IV drip (slowly), No. 10
- Thiogamma = thioctic acid;
- Vitamin B products (Milgamma) IM No. 10, or tablets (Berocca, Neurovit).
- Neuromidin, starting from 0.5 tab. TID for 2–3 days, followed by 1 tab. TID (1–2 months).
- Melsmon — 2 amp. (subcutaneously)
- Platelet-reach plasma — twice per week (subcutaneously)
- Hypoxen.
- Botulinum therapy (BTA injections in the contralateral side (performed by the surgeon or neurologist)) (4).
As a rule, in case of partial injury to the nerve, its contusion with an instrument or thermal injury by the cautery, after 4 weeks the treatment effect will be notable.
We present clinical cases from our practice.
Cases
Clinical Case 1:
Patient A, 36 years old. Injury to the temporal branch of the facial nerve as a result of the thread lifting. (Fig.4)
The patient underwent a procedure of thread lifting of the middle 1/3 of the face. A few days after the procedure, a break/tear of the thread on the right side occurred, and an attempt to correct this complication resulted in the development of facial asymmetry. According to the doctor’s opinion, this situation was a result of an injury to the soft tissues of the face. He recommended watchful waiting for a period during which all undesirable changes were supposed to resolve without treatment. After 1 month of follow-up, right-sided facial neuropathy was diagnosed, and neurotropic therapy was started. It should be noted that all doctors with whom the patient communicated a) were professionals and the thread application procedure was technically correct, and b) they did their best to help the patient. Let’s analyse why an injury to the buccal branch of the facial nerve have occurred in this triangle? It is known that the buccal (third) branch innervates zygomatic major and minor muscles, levator labii superioris, levator anguli oris, buccal muscle, orbicularis oris, nasal muscle, risorius muscles. Their injury often occurs simultaneously, and given that the zygomatic and buccal branches have mutual connections, muscle paralysis is rarely total. Although, in some cases, persistent deformity is possible, which is difficult to correct. In what cases this situation is possible? Injury to the zygomatic and buccal branches of the facial nerve is possible during SMAS lifting, thread lifting, both at the time of application and extraction of threads, during Radiesse procedure, as well as botulinum neuroprotein injections. (K Watanabe, et al. Anatomy for Plastic Surgery of the Face, Head, and Neck, by Thieme Medical Publishers, Inc., 2016, с. 241.
S Standring et al. Gray’s Anatomy. The Anatomical Basis of Clinical Practice, 2016, 41th ed. Elsevier Limited, с. 2252.)
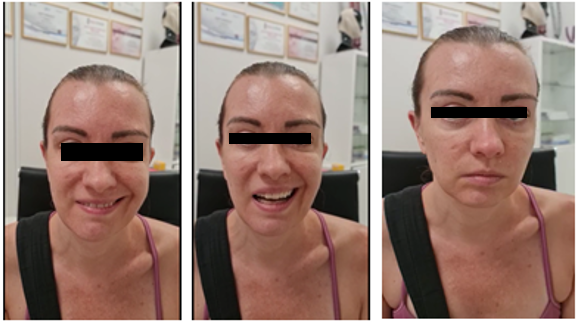
Figure 4. Clinical case of an injury to the zygomatic and buccal branches of the facial nerve
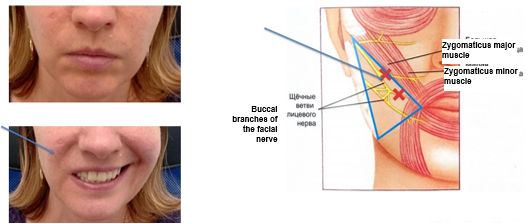
Figure 5. Neuropathy of the buccal and zygomatic branches of the facial nerve after thread lifting

Figure 6. Before and after botulinum toxin injections
Treatment:
- Thiogamma, 600 mg — IV drip, No. 10 (10 days).
- Milgamma — IM, No. 10 (10 days).
- Neuromultivit — 1 tab. BID (2 months).
- Botulinum therapy on the non-injured side in two sessions — 30 units.
- Melsmon — 4 ml subcutaneously along the course of the injured facial nerve trunks — 6 procedures.
- PRP along the middle 1/3 of the face — 4–6 procedures every 1–2 days.
- Consultation of neurologist.
- Physiotherapy: UHF therapy, microcurrents.
Clinical case 2:
Patient I, 40 years old. Injury of the temporal branch of the facial nerve as a result of the thread lifting. (Fig.7)
The patient underwent a thread lifting of the upper third of the face using the ‘Fox-Eye’ technique. 4 hours after the effect of anesthesia was supposed to finally resolve, on one side the eyebrow was mobile, and on the other side, mobility did not recover even within two weeks after the procedure. Upon admission neuropathy of the temporal branch of the facial nerve was diagnosed. The treatment was carried out according to the previously described protocol. Against the background of treatment, partial favourable changes were noted. Currently, the treatment is ongoing, correction of the iatrogenic persistent deficiency is planned using thread lifting or surgical methods.

Figure 7. Patient I, 40 years old. Injury of the temporal branch of the facial nerve as a result of the thread lifting procedure
Conclusion
Thus, facial nerve injury during thread lifting is a serious complication. Adequate and intensive treatment should be started as soon as possible, in the near hours after the development of clinical signs to ensure restoration of functions and reduce the duration of the rehabilitation period. It is mandatory to conduct treatment in cooperation with the neurologist.
References
- Edited by RJ Rohrich, JM Stuzin, E Dayana, EV Ross. Facial Danger Zones, 2022, 152 p.
View at Publisher | View at Google Scholar - Brooke R Seckel. Dangerous areas of the face, 2016, 52 p.
View at Publisher | View at Google Scholar - Alessio Redaelli. Dangerous areas of the face, how to avoid complications: simple rules for safe aesthetic correction, 2018, 66 p.
View at Publisher | View at Google Scholar - Ed. by Antonella Tosti, Kenneth Beer, Maria Pia de Padova (translated from English. under the general editorship by Prof. YaA Yutskovskaya). Treatment of complications after cosmetic procedures, 2014, 142 p.
View at Publisher | View at Google Scholar - Frank G Netter (translated from English. edited by Prof. AN Bogolepova). Cranial nerves, 2020, 154 p.
View at Publisher | View at Google Scholar - Hee Jin Kim, Kyle K. So, Hong-Ki Lee, Chisu Kim (translated from English, ed. by IE Khrustaleva). Clinical anatomy of the face for contour plastic surgery with fillers and botulinum toxin, 2018, 189 p.
View at Publisher | View at Google Scholar - AA Vorobyev et al. Cosmetological anatomy of the face of ALBI-St. Petersburg, 2017, 65–76 pp.
View at Publisher | View at Google Scholar - SV Surovykh, OR Orlova, AI Nerobeev et al., Facial nerve injury in plastic surgery. Annals of Plastic, Reconstructive and Aesthetic Surgery, 2011; N 1.- 8–30 pp.
View at Publisher | View at Google Scholar - OR Orlova, MA Akulov, DYu Usachev et al., The use of botulinum toxin type A in the acute period of facial nerve injury after neurosurgical interventions.
View at Publisher | View at Google Scholar
