

Research Article | DOI: https://doi.org/10.31579/2834-8427/046
Care of Traumatic Spinal Cord Injury Patients in Rural Population of India: An Analysis
1 M.B.B.S. D.N.B. Consultant Orthopaedic,Trauma & Joint Replacement Surgeon, Reliable Multispeciality Hospitaland Research Center, Nagpur India-440024.
2 M.B.B.S. D Ortho. Consultant Consultant Orthopaedic,Trauma & JointReplacement Surgeon, Reliable Multispeciality Hospital and Research Center, Nagpur India-440024.
3 M.B.B.S.M. D., Senior Consultant & Specialist Crictical Care, Reliable Multispeciality Hospitaland Research Center, Nagpur India-440024.
4 M.B.B.S.M.S Senior ResidentReliable Multispeciality Hospitaland Research Center,Nagpur. India -440024.
*Corresponding Author: B. Sanjay Ramchandra., M.B.B.S. D.N.B. Consultant Orthopaedic,Trauma & Joint Replacement Surgeon Reliable Multispeciality Hospital and Research Center, Nagpur India-440024.
Citation: B. Sanjay Ramchandra, Kawale swapnil, Sachin V Jibkate, Shraddha Nandurkar, (2025), Research Article: Care of Traumatic Spinal Cord Injury Patients in Rural Population of India: An Analysis., J Clinical Gynaecology and Breast, 4(6); DOI: 10.31579/2834-8427/046
Copyright: © 2025 B. Sanjay Ramchandra, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 November 2025 | Accepted: 14 November 2025 | Published: 26 November 2025
Keywords: spinal cord injury (SCI), spinal trauma centers, treatment outcome and rehabilitation, traumatic spinal cord injury
Abstract
Background: Management of spinal cord injured patients is an integral part of trauma care. There is needto congregate these patients in spinal trauma centers where facilities exist for better treatment outcome and rehabilitation. The objective of this study therefore, is to know how traumatic spinal cord injury patients are being treated at rural area of India and to suggest steps to improve the quality of care of the traumatic spinal cord injury patients in rural population of the Indian setup.
Materials and Methods: Sixty patients of traumatic spinal cord injury patients admitted between February 2024 and February 2025 were included in the study and their data was analyzed.
Results: Forty-seven (78.3%) of the spinal cord injured patients were males and the mean age was 35years (range 18-65 years). Thirty-eight (63.33%) of the spinal injuries occurred due to Road traffic accidents. There was an average of 10.75 days (range 3 hours-42 days) of delay in presentation to spinal trauma center and most of the time the cause for the delay was financial constraint on the part of patients. In 48 (80%) cases, the mode of transportation of the spinal cord injured patient to spinal trauma center was ambulance and attendants of the patient did not have any knowledge about precautions essential for transportation of spinal cord injured patients to prevent neurological deterioration. 11(18.3%) cases were given injection solumedrol. Forty- nine (81.7%) patients were treated nonoperatively and 11(18.3%) patients were treated by surgery. One (12.5%) patientof upper cervical region and two (25%)patients of lower cervical region where anterior cervical platting was done. One (12.5%) of lower dorsal and two (25%) patients of dorsolumbar region were pedicular screw fixation was done.Five (62.5%) patients of lumbosacral region were pedicular screw fixation was done.
Conclusion: For better outcome we re-emphasize the need to establish and congregate these patients into spinal trauma centers. We also suggest a social legislation, which will be fundamental to social re-integration of these SCI and other severely disabled patients.
Introduction
Spinal cord injury (SCI) is the most devastating event that can occur in an individual’s life, leading to long term disability and high rate of mortality. Despite the ongoing research in the treatment of spinal cord injury (SCI) this condition is not yet amenable to complete restoration of function, which is a big obstacle in independent living of the victim. Often spinal cord injured patientsare of the younger age group. (17) Most of these patients are managed at centers without spinal trauma center. The physical, personal, financial and social impact of spinal cord injury is such that most patients are lost in follow-up or succumb to life- threatening complications associated with spinal cord injury. However, inadequate precautions during transportation can cause further injury to the already compromised spinal cord in spinal injured patients. (3,15) Early surgery and comprehensive rehabilitation markedly reduces the overall morbidity of spinal cord injured patients by enabling the patient to lead an independent life. (6,8,14)
The larger number of patients managed in spinal trauma centers permit the staff to develop greater expertise and allow more cost-effective use of resources. Furthermore, it can provide adequate number of patients for clinical trials for research in the field. (14) Since there is no study available which discusses the problems faced by spinal cord injured patients in rural population of India, this study was conducted to assess such problems and to analyze them in order to make improvements in the present Indian setup.
MATERIALS AND METHODS
Sixty patients of traumatic spinal cord injury patients admitted between February 2024 and February 2025 were included in the study. Patients were included as per ASIA Grade.
Out of 60 patients, eight patients (13.3%) had upper cervical spine injuries (C1-C3), eight (13.3%) patients had lower cervical spine injuries (C4-C7), 6(10%) patients had upper dorsal spine injuries (D1-D6), 20 (33.3%) patients had lower
dorsal (D7-D11) and10(16.7%) patient had dorsolumbar spine (D12-L1) injuries and eight (13.3%) patients had lumbar and sacral spine injuries.
Out of 60 patients, 37(61.7%) patients were neurologically complete (ASIA Grade A), 12(20%) were neurologically incomplete (ASIA Grade B) and 11(18.3%) patients were ASIA Grade C.
Data was collected regarding patients age,sex, mode of injury, delay in presentation to spinal trauma center, cause for the delay in presentation to spinal trauma center, mode of transportation to hospital, precautions taken during transportation (paramedical personal accompanied the patient) to the hospital and treatment they received before
coming to the spinal trauma center. Data was analyzed using Epienfo.
Results
Forty-seven (78.3%) of the spinal cord injured patients were males and thirteen (21.7%) were females. The mean age of males was 35 years (range 18-65 years) and the mean age of females was 37 years (range 20-70 years). The mean age of the total study group was 36 years (range 18-70 years).
Out of 60, Road traffic accidents contributed for 38 (63.33%) cases. Fall of heavy object on the back accounted for seven (11.7%) cases.11 (18.3%) were due to fall from a tree, four (6.7%) duet to fall in drunken state from staircase.
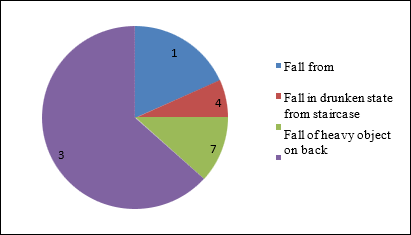
(Figure 1)
In 26 (43.3%) cases admitted to spinal trauma center up to 8 hours (mean 4.23 hours),18 (30%) cases admitted to spinal trauma center between 8-24 hours (mean 20.11 hours),7(11.7%) cases between 25 hours to one week (7 days (mean 6 days) and nine cases got admitted between one week to seven weeks (mean 35 days). There was an average of 10.75 days (range 3 hours-40 days) of delay in presentation to spinal trauma center and most of the time the cause for the delay was financial constraint. In 30 (50%) cases financial constraint was the reason for delay in presentation, whereas in thirteen (21.7%) cases reason for delay was the attendants did not have any information regarding the existence of spinal trauma centers. In 11(18.3%) cases reason for delay was the attendants were not informed till admission and six (10%) cases were from remote place where transportation facilities are lacking.
In 48 (80%) cases, the mode of transportation of the spinal cord injured patient to spinal trauma center was ambulance.6 (10%) cases, the mode of transportation was car and 6(10%) cases, the mode of transportation was lorry. Out of 60, admitted cases to spinal trauma center 39 (65%) accompanied by paramedical have knowledge about precautions essential for transportation of spinal cord injured patients to prevent neurological deterioration.21(35%) cases attendants of the patient or the transporting authority did not have any knowledge about precautions essential for transportation of spinal cord injured patients to prevent neurological deterioration.
Out of 60, twenty-one (35%) cases received treatment at local nursing home,10(16.7%) received native treatment.11(18.3%) cases were given injection solumedrol. 18(30%) cases were admitted to spinal trauma center without any treatment.
The patients were nursed on water mattresses, with instructions of absolute bed rest for Dorsolumbosacral injuries {44 patients (83.83%)}. Sixteen patients with cervical spine injuries were managed with crutchfield tong, and cervical collar. Supportive care like chest physiotherapy, pelvic bridging exercises were carried out.
Out of 60, forty- nine (81.7%) patients were treated nonoperatively and 11(18.3%) patients were treated by surgery. Out of 11 (18.3%) patients treated surgically, one (12.5%) patient of upper cervical region and two (25%) patients of lower cervical region where anterior cervical platting was done. One (12.5%) of lower dorsal and two (25%) patients of Dorsolumbar region were pedicular screw fixation was done. Five (62.5%) patients of lumbosacral region were pedicular screw fixation was done.
Discussion
Management of spinal cord injured patients in spinal units with dedicated experts and facilities for comprehensive rehabilitation improves the outcome. (9) Comprehensive rehabilitation team of spinal trauma unit involves team work involving various specialists including vocational evaluator and a social worker.
Males were found to be more prone for spinal cord injury in our series, which is similar to findings in other studies as they are more engaged in outdoor work and hence are more prone for spinal cord and/or other trauma. (2,5,7,9,14-17) Our study also reflects the adult population being the most susceptible for spinal injuries. Adult people are the active age group of any community, which makes them more susceptible for spinal cord injuries. The mean ages of patients of SCI reported are from 30.9 years - 38.9 years from various series. (3,4,8,10,13.14)
In Nigeria, the most common cause for spinal cord injury was road traffic accidents, as reportedby Solagberu.(4)Otomet al.,(16) reported that in Jordan, most spinal cord injuries resulted from road traffic accidents. In India, the most common cause for spinal cord injury was fall from height followed by road traffic accidents, as reported by Pandey et al. (17) Possible cause of variation could be houses in rural and urban areas lack essential safety precautions like fencing of the terrace and guarding of the staircase, thereby making fall from height a realistic possibility in study of Pandey et al. (17)
Lack of strict implementation of traffic rules in various nonmetropolitan cities of India along with lack of awareness among the general population regarding adherence to traffic rules still prevails as an important cause of road traffic accident and spinal trauma.
Early presentation of spinal injured patients to a spinal unit enables early surgery, which is beneficial in terms of reducing complications, length of stay and hospital cost. (6) Scivoletto(4) concluded that spinal injured patients presenting early at spinal unit show better functional outcome after rehabilitation than patients presenting late. It is obvious from the results of the study that spinal cord injured patients. In India present quite late at specialized spinal units and the cause for the delay in most cases was unawareness on part of patient/patient’s attendants regarding existence of such spinal trauma center. Delayed presentation to spinal center adversely affects the final functional outcome of the patient after rehabilitation. (10)
Expeditious and careful transport of patients with acute cervical spine or spinal cord injuries should be carried out from the site of injury by the most appropriate mode of transportation available to the nearest capable definitive care medical facility. (15) In a study conducted by Burney et al (2) it was reported that more than half of spinal cord injured patients were transported by air, in Michigan. In our study we found that patients were mode of transportation was ambulance (80%).
Moreover, attendants accompanying such patients had little knowledge regarding precautions to be taken to prevent further neurological deterioration during transportation.
A study conducted by Yu et al (16) reported that early repeated methylprednisolone sodium succinate treatment might allow greater recovery from acute spinal cord injury. Sharma etal(11)suggested that methylprednisolone sodium succinate was effective in promoting post-traumatic clinical and histological recovery and to a greater extent, when given 1h after trauma. Methylprednisolone sodium succinate is more effective than dexamethasone in reducing edema when both are given after an interval of 1h. (11) In our study we found that only eleven (18.3%) spinal cord injured patients received injection solumedrol.
Recommendations from a study conducted by Surkin et al (13,17) for prevention of spinal cord injury, like increasein safety belt usage, increasing alcohol awareness andreducing violence should also be implemented in India.Print, electronic and radio media should be used toemphasize prehospital care, precautions for transportationof spinal cord injured patients, and availability of tertiarylevel spinal trauma centers for financially weaker sections ofthe society.
Medical and paramedical staff across the country is still quite unaware about the socioeconomic impact of spinal cord injuries. Training programs to give an opportunity to health workers to improve their knowledge in the comprehensive management of spinal cord injured patientsshould be carried out on a regular basis. (14) Hospitals managing spinal cord injured patients must have a comprehensive spinal trauma patient rehabilitation team. Complications associated with spinal cord injuries must be addressed immediately with help of specialists of other specialities like gasteroenterology, urology, plastic surgery, and general medicine. Every effort should be made to make spinal cord injured patients independent and put them back into mainstream.
A suggestion from a study conducted by Nwadinigweet al (6) stressed upon the need to congregate spinal injured patients into regional spinal centers. The study also suggested a social legislation, which will be fundamental to the social reintegration of these spinal cord injured patients. In India also, these suggestions should be given due importance so that spinal cord injured patients, after proper rehabilitation, can become part of the mainstream population.
There is a need to set up more specialized spinal trauma centers across the country with good accessibility to poorer sections of society for comprehensive management of spinal cord injured patients. Early liaison of hospitals without specialized spinal trauma centers to specialized spinal trauma centers should be encouraged, so that early presentation of acute spinal cord injured patient to a specialized spinal trauma center leading to early surgery and comprehensive rehabilitation can be carried out.(10,17) Kishan et al(4) emphasized that early surgical treatment is beneficial in terms of reducing complications, length of stay and hospital costs.(4)Fehling and Perrin(3) suggested that urgent decompression in acute cervical spinal cord injury remains a reasonable practice option and can be performed safely.
Early decompression and stabilization of injured spinal cord is an area that is still overlooked in the Indian setup. This is quite evident from our study in which only 18.4% of the patients were decompressed and stabilized, early decompression and stabilization of injured spinal cord is an area that is still overlooked in the Indian setup.
Job reservations should be encouraged for spinal cord injured patients. The home visit program conducted at Ahmadabad by Prabhaka and Thakkar (9) for spinal cord injured patients decreased the number of re-admissions by improving the status of rehabilitation, which raised the quality of care for patients with spinal cord injury. Such programs can be carried on a broader basis like national programs, so that maximum numbers of spinal cord injured patients are benefitted.
Our study has the limitation that it was conducted at spinal trauma center lacking facilities of a tertiary level spinal center in a metropolitan city.
Conclusion
For better outcome of SCI, we re-emphasize the need to establish and congregate these patients into spinal trauma centers. We also suggest a social legislation, which will be fundamental to social re-integration of these SCI and other severely disabled patients.
Competing interests
“The author(s) declare that they have no competing interests”.
Consent
patient has given their informed consent for the case report to be published.
Financial Support and Sponsorship
Nil.
References
- Amin A, Bernard J, Nadarajah R, Davies N, Gow F, Tucker S. Spinal injuries admitted to a specialist hospital centre over a 5- year period: A study to evaluate delayed admission. Spinal Cord 2005; 43:434-7.
View at Publisher | View at Google Scholar - Burney RE, Waggoner R, Maynard FM. Stabilization of spinal cord injury for early trasfer. J Trauma 1989; 29:1497-9
View at Publisher | View at Google Scholar - Fehling MG, Perrin RG. The role and timing of early decompression for cervical spinal cord injury: Update with a review of recent clinical evidence. Injury 2005;36: B13-26
View at Publisher | View at Google Scholar - Kishan S, Vives MJ, Reiter MF. Timing of surgery following spinal cord injury. J Spinal Cord Med 2005; 28:11-9
View at Publisher | View at Google Scholar - Kovindha A, Dollfus P. Workshop on spinal cord injuries (SCI) management: The Chiang Mai experience. Spinal Cord 1999; 37:218-20.
View at Publisher | View at Google Scholar - Nwadinigwe CU, Iloabuchi TC, Nwabude IA. Traumatic spinal cord injuries (SCI): A study of 104 cases. Niger J Med 2004; 13:161-5.
View at Publisher | View at Google Scholar - O’Connor RJ, Murray PC. Review of spinal cord injuries in Ireland. Spinal Cord 2005 Nov 22.
View at Publisher | View at Google Scholar - Otom AS, Doughan AM, Kawar JS, Hattar EZ. Traumatic spinal cord injuries in Jordan--an epidemiological study. Spinal Cord 1997; 35:253-5.
View at Publisher | View at Google Scholar - Prabhakar MM, Thakkar TH. A follow-up programme in India for patients with spinal cord injury: Paraplegia safari. J Spinal cord Med 2004:27:260-2
View at Publisher | View at Google Scholar - Scivoletto G, Morganti B, Molinari M. Early versus delayed inpatient spinal cord injury rehabilitation: An Italian study. Arch Phys Med Rehabil2005; 86:512-6.
View at Publisher | View at Google Scholar - Sharma A, Tiwari R, Badhe P, Sharma G. Comparison of methylprednisolone with dexamethasone in treatment of acute spinal injury in rats. Indian J Exp Biol 2004; 42:476-80.
View at Publisher | View at Google Scholar - Solagberu BA. Spinal cord injuries in Ilorin, Nigeria. West Afr J Med 2002; 21:230-2.
View at Publisher | View at Google Scholar - Surkin J, Gilbert J, Harkey HL 3rd, Sniezek J, Currier M. Spinal cord injury in Mississippi. Findings and evaluation, 1992-1994. Spine 2000; 25:716-21.
View at Publisher | View at Google Scholar - Tator CH, Duncan EG, Edmonds VE, Lapczak LI, Andrews DF. Neurological recovery, mortality and length of stay after acute spinal cord injury associated with changes in management. Paraplegia 1995; 33:254-62.
View at Publisher | View at Google Scholar - Transportation of patients with acute traumatic cervical spine injuries. Neurosurgery 2002;50: S18-20.
View at Publisher | View at Google Scholar - Yu Y, Matsuyama Y, Nakashima S, Yanase M, Kiuchi K, Ishiguro N. Effects of methylprednisolone sodium succinate (MPSS) and a potent inducible nitric oxide synthetase (iNOS) inhibitor on traumatic spinal cord injury. Neuroreport 2004; 15:2103-7.
View at Publisher | View at Google Scholar - VK Pandey, V Nigam, T Goyal D, HS ChhabraCare of post- traumatic spinal cord injury patients in India: An analysis:Indian j Ortho,v 41(4) oct 2007
View at Publisher | View at Google Scholar
