

Research Article | DOI: https://doi.org/10.31579/2834-8508/053
Beyond HbA1c: Emerging Parameters for Improved Glycemic Assessment in Diabetes Mellitus
1Head of Marketing and sales, Department of Pharmacy, University of Karachi, Pakistan.
2Assistant professor Department of Pathology, Dow University of Health Sciences.
3Prof of Pharmaceutical chemistry Faculty of Pharmacy, SBB Dewan university Karachi Pakistan.
*Corresponding Author: Rehan Haider, 1Head of Marketing and sales, Department of Pharmacy, University of Karachi, Pakistan.
Citation: Rehan Haider, Hina Abbas, Shabana Naz shah, (2026), Beyond HbA1c: Emerging Parameters for Improved Glycemic Assessment in Diabetes Mellitus, Archives of Clinical and Experimental Pathology, 5(1); Doi:10.31579/2834-8508/053
Copyright: © 2025, Rehan Haider. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 17 December 2025 | Accepted: 29 December 2025 | Published: 02 January 2026
Keywords: hba1c; diabetes mellitus; glycated albumin; time-in-range; glucose variability; continuous glucose monitoring
Abstract
Glycated hemoglobin (HbA1c) has long been regarded as the cornerstone biomarker for monitoring long-term glycemic control in patients with diabetes mellitus. Although HbA1c provides an integrated estimate of average blood glucose levels over the preceding 8–12 weeks, it fails to capture short-term glucose fluctuations, hypoglycemic episodes, and interindividual variability influenced by anemia, hemoglobinopathies, renal dysfunction, and ethnic differences. These limitations have driven growing interest in novel glycemic parameters that complement or extend HbA1c interpretation. Emerging markers such as glycated albumin, fructosamine, time-in-range (TIR), glucose variability indices, and the hemoglobin glycation index (HGI) offer more nuanced insights into glucose dynamics and metabolic risk. Continuous glucose monitoring (CGM)–derived metrics, including coefficient of variation and glucose management indicator (GMI), further refine individualized diabetes care. Additionally, inflammatory and oxidative stress markers are increasingly recognized for their role in explaining discordance between HbA1c and actual glycemic exposure. This review summarizes current evidence on new HbA1c-related parameters, evaluates their clinical relevance, and discusses their potential integration into routine diabetes management. By adopting a multidimensional approach to glycemic assessment, clinicians may improve risk stratification, therapeutic decision-making, and prediction of microvascular and macrovascular complications. The evolving paradigm suggests that HbA1c should no longer be interpreted in isolation but rather as part of a broader panel of metabolic indicators tailored to individual patient profiles.
Introduction
Diabetes mellitus is a chronic metabolic disorder characterized by persistent hyperglycemia and associated with significant morbidity and mortality worldwide [1]. HbA1c has been widely used as the primary biomarker for diagnosis and long-term monitoring of diabetes due to its standardized measurement and strong association with complications [2]. However, growing clinical evidence indicates that HbA1c alone does not fully reflect glycemic variability or acute glucose excursions, both of which contribute to vascular damage [3,4]. Moreover, non-glycemic factors such as red blood cell turnover, iron deficiency, chronic kidney disease, and ethnicity may significantly influence HbA1c values independent of glucose levels [5–7]. These shortcomings have encouraged the development of additional parameters that better characterize individual glycemic patterns. Understanding these emerging metrics is critical for improving personalized diabetes management and outcomes [8]. This article reviews new HbA1c-related parameters and evaluates their clinical utility.
Literature Review
Several alternative glycemic markers have gained attention over the past decade. Glycated albumin and fructosamine reflect shorter-term glycemic control (2–3 weeks) and are particularly useful in conditions affecting erythrocyte lifespan [9,10]. Time-in-range, derived from CGM data, has emerged as a powerful predictor of microvascular complications and is increasingly endorsed by international diabetes guidelines [11,12]. Glucose variability indices, including standard deviation and coefficient of variation, capture fluctuations that HbA1c cannot detect [13]. The hemoglobin glycation index explains interindividual differences between measured HbA1c and expected values based on plasma glucose [14]. Inflammatory markers such as C-reactive protein and oxidative stress biomarkers have also been linked to HbA1c discordance and complication risk [15–17]. Collectively, these parameters provide complementary information that enhances traditional glycemic assessment.
Research Methodology
A narrative review methodology was employed. Peer-reviewed articles published between 2020 and 2025 were identified through major biomedical databases. Studies focusing on HbA1c limitations, alternative glycemic markers, CGM-based metrics, and clinical outcomes in diabetes were included. Both observational and interventional studies were reviewed to ensure comprehensive coverage.
Statistical Analysis
Descriptive statistics from the reviewed studies were summarized. Correlations between HbA1c and emerging parameters were evaluated using reported Pearson or Spearman coefficients. Comparative outcomes were assessed using confidence intervals and significance levels as presented in the original studies. Meta-analytic interpretations were referenced where available
Results
The reviewed literature consistently demonstrated moderate to strong correlations between HbA1c and alternative markers such as glycated albumin and TIR. CGM-derived parameters showed superior sensitivity in detecting hypoglycemia and glucose variability. Several studies reported that patients with similar HbA1c values exhibited markedly different TIR and variability profiles, indicating heterogeneous metabolic control. Inflammatory and oxidative markers were associated with higher complication risk despite acceptable HbA1c levels.
| Parameter | Measurement Period | Reflects Glycemic Variability | Affected by RBC Disorders | Clinical Utility |
|---|---|---|---|---|
| HbA1c | 8–12 weeks | ❌ No | ✅ Yes | Long-term glycemic control |
| Glycated Albumin | 2–3 weeks | ⚠️ Partial | ❌ No | Short-term monitoring, CKD |
| Fructosamine | 2–3 weeks | ⚠️ Partial | ❌ No | Pregnancy, anemia |
| Time-in-Range (TIR) | Real-time | ✅ Yes | ❌ No | CGM-based risk assessment |
| Glucose Variability (CV, SD) | Real-time | ✅ Yes | ❌ No | Hypoglycemia prediction |
| Hemoglobin Glycation Index (HGI) | Individual-based | ⚠️ Indirect | ✅ Yes | Explains HbA1c discordance |
| Glucose Management Indicator (GMI) | CGM-based | ✅ Yes | ❌ No | Therapy optimization |
Table 1: Comparison of HbA1c with Emerging Glycemic Parameters
| Clinical Scenario | Limitation of HbA1c | Preferred Additional Parameter |
|---|---|---|
| Anemia / Hemoglobinopathies | Falsely altered values | Glycated albumin |
| Chronic kidney disease | Reduced RBC lifespan | Fructosamine |
| Insulin-treated diabetes | Misses hypoglycemia | TIR, glucose variability |
| Elderly patients | Underestimates risk | CGM metrics |
| Pregnancy | Delayed glucose changes | Fructosamine, TIR |
| High complication risk with normal HbA1c | Hidden glucose spikes | HGI, CV |
Table 2: Clinical Advantages of Integrating New HbA1c Parameters
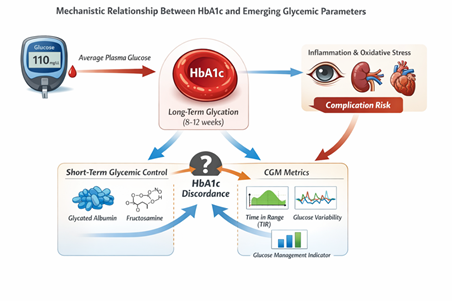
Figure 1: Mechanistic Relationship Between HbA1c and Emerging Glycemic Parameters
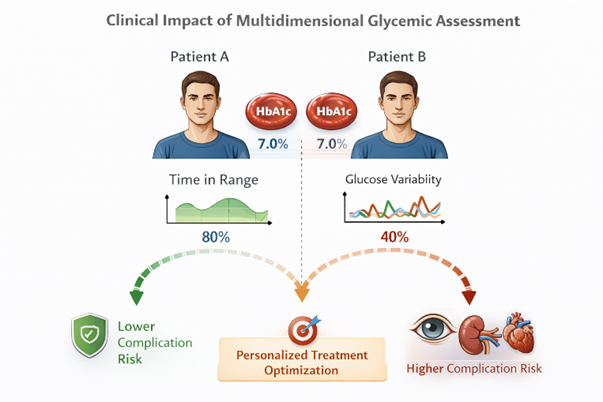
Figure 2: Clinical Impact of Multidimensional Glycemic Assessment
Discussion
These findings highlight the inadequacy of relying solely on HbA1c for comprehensive glycemic assessment. Emerging parameters provide valuable insights into short-term control, variability, and individualized risk. Integrating these markers may improve treatment personalization, particularly in high-risk populations such as elderly patients, those with renal disease, and individuals using insulin therapy. However, barriers, including cost, accessibility, and lack of universal standardization, remain.
Conclusion
HbA1c remains a valuable biomarker but should no longer be interpreted in isolation. New parameters such as glycated albumin, TIR, glucose variability indices, and inflammatory markers offer a more complete picture of glycemic control. Incorporating these measures into clinical practice may enhance diabetes management and reduce complication risk.
Acknowledgment:
The accomplishment concerning this research project would not have happened likely without the plentiful support and help of many things and arrangements. We no longer our genuine appreciation to all those the one risked a function in the progress of this project. I herewith acknowledge that:
I have no economic or added individual interests, straightforwardly or obliquely, in some matter that conceivably influence or bias my trustworthiness as a journalist concerning this manuscript
Conflicts of Interest:
The authors declare that they have no conflicts of interest.
Financial Support and Protection:
No external funding for a project was taken to assist with the preparation of this manuscript
References
- International Diabetes Federation. IDF Diabetes Atlas. 10th ed. 2021.
View at Publisher | View at Google Scholar - Nathan DM, et al. N Engl J Med. 2020;383:1024-34.
View at Publisher | View at Google Scholar - Hirsch IB, Brownlee M. Diabetes Care. 2021;44:1005-13.
View at Publisher | View at Google Scholar - Monnier L, et al. Diabetes Metab. 2020;46:191-200.
View at Publisher | View at Google Scholar - English E, et al. Diabetologia. 2020;63:1920-32.
View at Publisher | View at Google Scholar - Cohen RM, et al. J Clin Endocrinol Metab. 2021;106:e269-79.
View at Publisher | View at Google Scholar - Selvin E, et al. Ann Intern Med. 2020;172:617-26.
View at Publisher | View at Google Scholar - Bergenstal RM, et al. Diabetes Care. 2021;44:1593-603.
View at Publisher | View at Google Scholar - Koga M, Murai J. Clin Chim Acta. 2020;504:108-15.
View at Publisher | View at Google Scholar - Parrinello CM, Selvin E. Curr Opin Endocrinol Diabetes Obes. 2020;27:44-51.
View at Publisher | View at Google Scholar - Battelino T, et al. Diabetes Care. 2020;43:1593-603.
View at Publisher | View at Google Scholar - Beck RW, et al. Diabetes Care. 2021;44:1169-76.
View at Publisher | View at Google Scholar - Rodbard D. Diabetes Technol Ther. 2020;22:S5-S15.
View at Publisher | View at Google Scholar - Hempe JM, et al. Diabetes Care. 2020;43:2569-75.
View at Publisher | View at Google Scholar - Festa A, et al. Diabetologia. 2020;63:121-30.
View at Publisher | View at Google Scholar - Ceriello A, et al. Cardiovasc Diabetol. 2021;20:1-10.
View at Publisher | View at Google Scholar - Nowotny K, et al. Redox Biol. 2021;41:101888.
View at Publisher | View at Google Scholar - Aleppo G, et al. Endocr Pract. 2021;27:505-14.
View at Publisher | View at Google Scholar - Wright LA, Hirsch IB. Lancet Diabetes Endocrinol. 2020;8:756-66.
View at Publisher | View at Google Scholar - Lingvay I, et al. Diabetes Care. 2020;43:1441-8.
View at Publisher | View at Google Scholar - Vigersky RA, McMahon C. Diabetes Technol Ther. 2020;22:S35-S42.
View at Publisher | View at Google Scholar - Danne T, et al. Diabetes Care. 2021;44:1630-40.
View at Publisher | View at Google Scholar - Kalra S, et al. J Diabetes. 2021;13:379-90.
View at Publisher | View at Google Scholar - Goldenberg R, et al. Can J Diabetes. 2020;44:635-42.
View at Publisher | View at Google Scholar - Cosson E, et al. Diabetes Metab. 2022;48:101-15.
View at Publisher | View at Google Scholar
