

case Report | DOI: https://doi.org/10.31579/ 2834-8532/062
An Unusual Cause of Diastolic Restriction and Pulmonary Hypertension: Pulmonary Hydatid Cyst Associated to Pulmonary Embolism- A Rare Association
- Tamir el M 1*
- Amri M 1
- Al timimi A 1
- Pr haboub M 1
- Pr Drighil A 1
- Pr Habbal R 1
- Dr soussi O 2
- Ouamer FZ 2
- Pr Merzem A 2
- Pr Belgadir H 2
- Pr moussali N 2
- Pr Benna N 2
1. Cardiology Department of Ibn Rochd University Hospital of Casablanca.
2. Radiology Department of Ibn Rochd University Hospital.
*Corresponding Author: Tamir el M, Universidad de la Salud, Mèxico.
Citation: : Tamir el M, Amri M, Al timimi A1, Pr haboub M, Pr Drighil A, Pr Habbal R, Dr soussi o, Ouamer FZ, Pr Merzem A, Pr Belgadir H, Pr moussali N, Pr Benna N, (2025), An Unusual Cause of Diastolic Restriction and Pulmonary Hypertension: Pulmonary Hydatid Cyst Associated to Pulmonary Embolism- A Rare Association, Clinical Genetic Research; 4(6): DOI: 10.31579/ 2834-8532/062
Copyright: © 2025 Tamir el M, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 December 2025 | Accepted: 15 December 2025 | Published: 26 December 2025
Keywords: pulmonary hypertension; pulmonary embolism; diastolicdys function; respiratory symptoms
Abstract
Pulmonary hydatid disease, attributable to *Echinococcus granulosus*, is prevalent in various regions, notably among rural populations in Mediterranean countries. The condition frequently manifests with respiratory symptoms, but can also result in systemic issues, particularly when cysts exert pressure on neighboring structures, including the heart. This report examines an uncommon correlation between pulmonary hydatid cysts, pulmonary embolism, diastolicdys function, and pulmonary hypertension.
Case Presentation
A 57-year-old woman from a rural community with a documented history of pulmonary hydatid disease presented to our clinic with chronicdyspnea, persistent cough, unintentional weight loss, and clinical indications of right ventricular dysfunction. Imaging studies, comprising chest X-ray, CT scan, and transthoracic echocardiography, identified bilateral pulmonary embolism alongside substantial mediastinal hydatid cysts that were compressing the heart. These cysts induced hemodynamic alterations, characterized by increased pulmonary pressures and diastolic dysfunction.
Management and Outcome:
The patient was started on anticoagulation therapy with Apixaban to address the pulmonary embolism, and albendazole was recommended for the management of the hydatidcysts. Unfortunately, despite the proposed medical treatments, the patient refused surgical intervention and sadly passed away one month following the diagnosis.
Conclusion:
This case underscores the rare and intricate relationship between pulmonary hydatid cysts and pulmonaryembolism, which can lead to significant cardiovascular implications, including diastolic dysfunction and pulmonary hypertension. Timely diagnosis and suitable management— especiallysurgical options whenfeasible—are essential for enhancing patient prognosis. This case underscores the necessity of considering hydatid disease in the differentialdiagnosis of pulmonaryembolism, particularly in endemicregions.
Introduction
Human hydatid disease is endemic in Morocco and remains a health concerneproblem in Mediterranean countries. It occurswhen the tapeworm Echinococcus devellops through its metacestode stage to formlarvae. The majority of human infections are caused by E. granulosus which leads to cystic echinococcosis [1].
The primary hosts of the worm include dogs, wolves and coyotes, while sheep, cattle, and deer are considered as intermediate hosts. Humans can become infected through exposure to contaminated water, food, and direct contact with carnivorous animals: however, they do not participate in worm’s biological cycle. Residing in rural area isa significant risk factor that warrants further investigation.
The initial type is primary echinococcosis, which can panifest in anyorgan; the second type is secondary echinococcosis, characterized by the dissemination of metacestodes from primary locations to other areas [1].
The lungis the second organ most frequently affected, following the liver [2]. Intrathoracic extrapulmonary localizations may involve various structures, including the pleura, pericardium, diaphragm, and chest wall. [3].
Hydatidcysts can alsobelocated in other locations such as the kidneys and spleen, which occurs in approximatively 2% of cases [4]. Additionnaly, bones, muscles and the brain may alsobe affected by the infection.
The diagnosis of hydatid disease relies on characteristic clinical and radiologicalfindings.
In this report, wepresent a case of a pulmonary hydatid cyst that led to compressive cardiacpre-tamponnade, accompanied by pulmonary embolism which resulted in diastolic restricion and pulmonary hypertension. Weaim to elucidate the clinical and imaging manifestations with this condition.
Case Presentation
We present the case of a 57-year-old woman residing in a rural area. Her medical history incudes a pulmonary hydatid infection that occured twenty years prior, which was managed medically with a positive outcome.
The patient was admitted to our hospital presenting respiratory symptoms that included chronic dyspnea, a cough accompanied by hydatidoptysis, basithoracic pain,
and a sensation of heaviness. Additionnaly, shelost 4 kg of herweight over the course of one-month, nocturnal sweats, asthenia and significant severe anorexia.
Upon clinical assessment, the patient presented as hemodynamically fairly stable. However cardiovascular examination revealed signs of right ventriculardys function, along side notable finding of painful hepatomegaly comprising 35 finger spans, hepatojugular reflux and lower extremity edema. The pleuropulmonary examination
indicatged the presence of sub-crepitatingrales in the left basithoracic region.
The routine hematologicalexaminationreturned normal results; however, the D-dimer assayindicatedelevatedlevels.
A chest X-rayrevealed a significiant rounded opacity in the lefthemithorax, which obscured the outline of both the leftmediastinal border and the ipsilateral diaphragmatic dome, consistent with the silhouette sign and indicating its antero-inferior positioning. Additionnaly a similar opacity was identified in the right lower hemithorax. (Figure 1).

On a 12-lead electrocardiogram (ECG), sinus tachycardia accompanied by a secondary repolarization disorder was observed, along with the presence of ventricular premature complexes (Figure 2)

A computedtomography (CT) chest scan revealed (Figures 3-7):
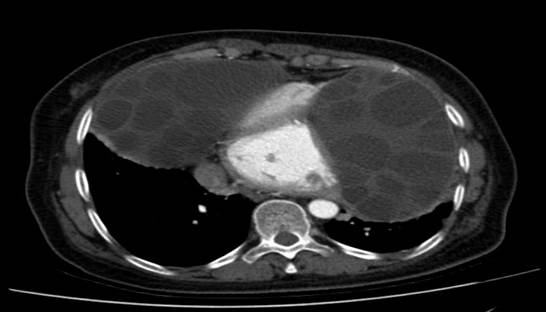

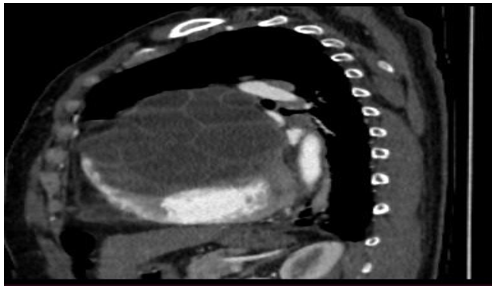


• Evidence of bilaterallobar and segmental pulmonaryembolism on the right in addition to segmental pulmonary embolism localized to the leftside. The seembolic changes exhibited a chronic appearance without any indication of pulmonary parenchymal infarction. (Figures 6-7). These finding scorrelated with the observed increase in D- dimer levels.
• 2 large bilater alanterior mediastinal and para- cardiac formations, likely of hydatid origin, are
causing extrinsic compression of the cardiaccavities (Figures 3 – 5):
The structures in question are characterized by multi-walls, a regular outline, distinct margins, and an enhanced wall definition following the injection of contrast medium.
The dimensions on the right are 93 x 114 mm and extend over 119 mm;whileon the left, the measurements are 119 x 78 mm extanding over 140 mm.
Posteriorly, these structures exertcompression on the adjacent lungparenchymaresulting in passive collapse.
• Absence of pleural effusion.
The transthoracic echocardiographic examination revealed (Figures 8 – 18):
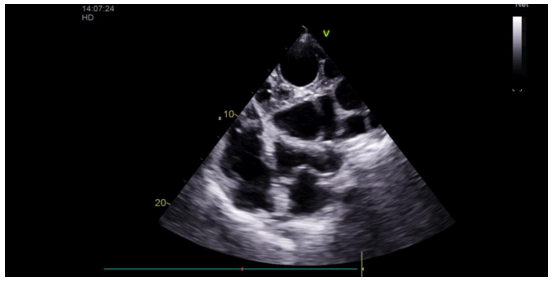

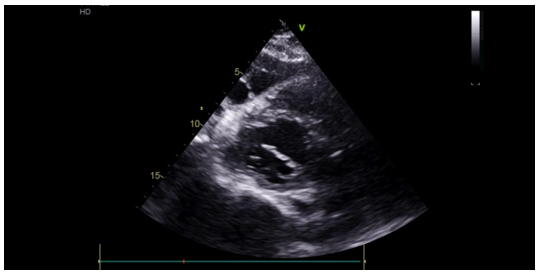
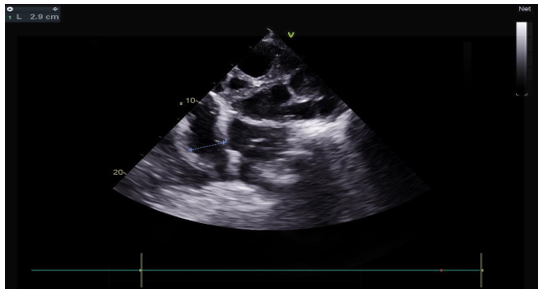
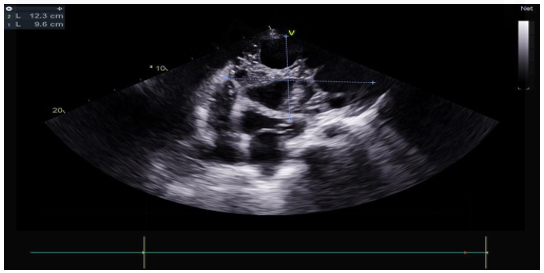
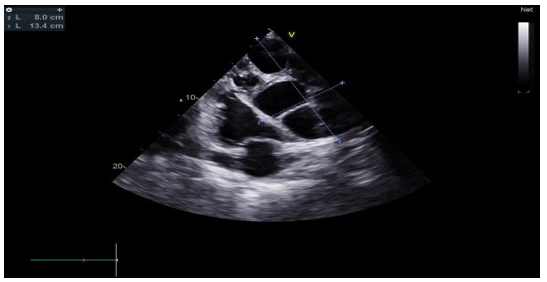
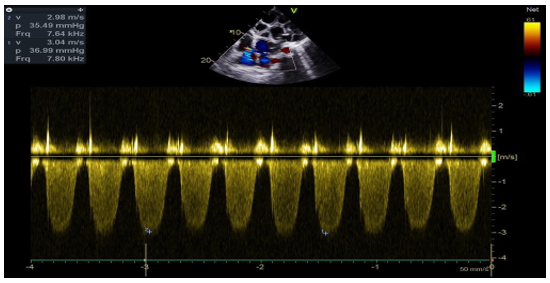
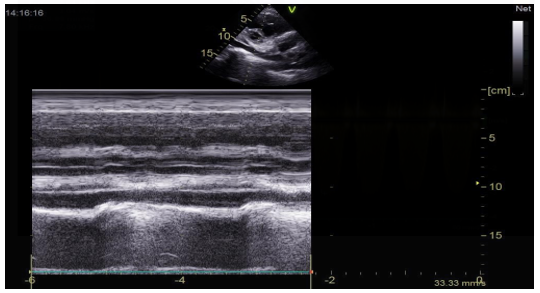
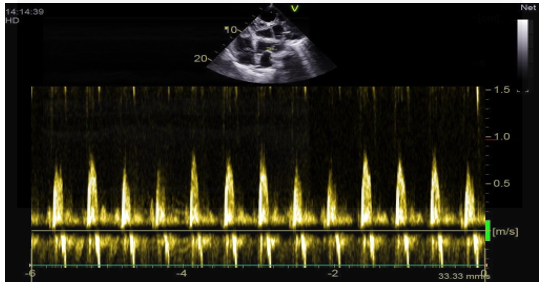
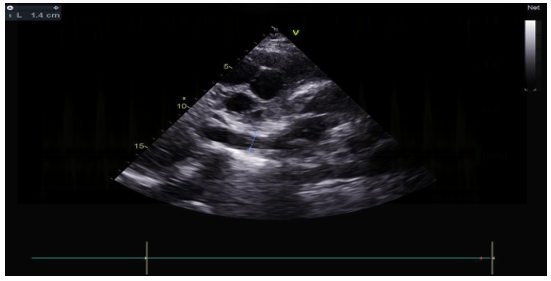
- A lobulatedcystic image exerting severe compression on both the right and left cardiac chambers, resulting in hemodynamic disturbance and considerable fluctuation in respiratory flows (Figures 12 – 13,17).
- Left ventricule showed no sign of dilatation. Al though the assessment of contractile function was influeced by compressio from pulmonary hydatid cyst, it appears to maintain functionnality.
- Elevated left ventricular filling pressure were noted.
- The right ventricle exhibited no dilation (Figure 11) despite the presence of longitudinal systolicdys functio n (Figures 14).
- Grade II tricuspid insufficiency was identified, with an estimated systolic pulmonary arterial pressure of 47 mmHg (calculated as 37 + 10 mmHg), indicating the presence of pulmonary hypertension.
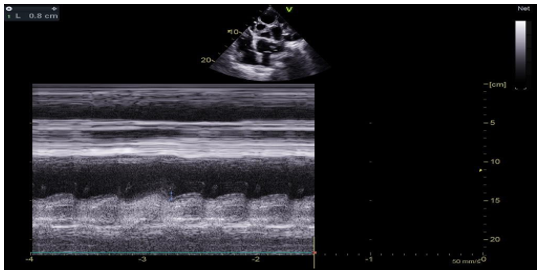
- The inferior vena cavademonstrated no dilation (Figure 18) and wasnoted to be non-compliant (Figure 16).
- No pericardial effusion was present.
No additionnal localized findings were identified during the abdominal ultrasound examination.
We maintained the diagnosis of cardiacpre-tamponade secondary to a large pulmonary hydatid which leaded to an a diastolism alongside pulmonary embolism.
The patient's respiratory and haemodynamic conditions were monitored, and she was initiated on anticoagulant therapy with APIXABAN.
The Surgical intervention was presented as a criticaloption to both the patient and herfamily ; however, they ultimately decided against undergoing the procedure. Consequently, we suggested a medical treatment regimen including ALBENDAZOLE, despite the factthat the hydatid cyst had not ruptured.
Regrettably, the patient passedaway one month following the diagnosis.
All procedures performed in this study were in accordance the ethical standards of the institutional and/or national research committee(s) and with the Helsinki Declaration (as revisedin 2013).
Discussion
Hydatiddiseaseis a widespread cyclo zoonotic infection that remains a significant public health concern, particularly in ruralregions. It is primarly caused by the parasites Echinococcus granulosus and Echinococcus multilocularis. This infection is endemic in various geographical areas, including the Mediterraneanregion, Africa, South America, the Middle East, Australia and New-Zealand. The most prevalent manifestation of hydatidosis in humans is cystic echinococcosis (CE). In this transmission cycle, dogs serve as definitive hosts whilesheepact as intermediate hosts.
The liver serves as the primary line of defense in humans, accounting for involvement in approximatively75 % of cases. In contrast, the lungs are implicatedin 15% of cases, as was observed in our patient, while other sites of involvement make up the remaining 10% [2].
Literatureindicatesthatmediastinallocalizationpredominantly occurs in the posterior mediastinum, withanterior and upper mediastinal presentations being comparatively rare. Notably, this type of localization tends to progress to calcification more frequently than pulmonary hydatid cysts, primarily due to the lack of ventilation-related factors [5].
This condition is predominantly asymptomatic; however, it can present with a range of symptoms due to its compressive impact on near by vital structures. Common manifestations include dyspnea, retrosternal chest pain, cough, dysphagia, back pain, and superior vena cava syndrome [6]. In the case of our patient, the symptoms were primarily a result of compression on the cardiac chambers.
The patient exhibited pulmonary hypertension as a result of pulmonary embolism and diastolic dysfunction due to compression from a hydatidcyst, despitesuch occurrences being exceptionally linked to Echinococcus granulosus infection. Symptoms such as cough, dyspnea, dysphagia, and chest pain are frequently documented in similar cases, mirroring the presentation of our patient [7].
The most significant complications include invasion of the aorta and the potential onset of anaphylactic shock resulting from an allergicreaction to the cyst [8].
Hydatid serology can offer valuable diagnostic insights in numerous cases and facilitate the assessment of treatment effectiveness [9].
Imaging techniques such as echocardiography, computed tomography (CT), and magneticresonanceimaging (MRI) are effective in visualizing the cysticcharacteristics of the mass and its relationship with the cardiac chambers.
Hydatidcysts are categorized into four distinct types based on their imaging characteristics:
- Type I (Simple cysts): These appear as well-defined, anechoic masses on ultrasound, which may contain hydatids and or septa. On computed tomography (CT), they display homogeneous fluid attenuation, whilemagneticresonanceimaging (MRI) shows low signal on T1-weighted images and high signal on T2- weighted images, typically accompanied by a darkrim on both imaging sequences.
- Type II (Cysts with daughter cysts and matrix): Daughter cysts manifest as smallercystic formations, usually located at the periphery of the primarycyst. These have a lower attenuation on CT and are iso- or hypointense compared to the matrix. In certain instances, larger, irregularly shaped daughter cysts can dominate the interior of the primarycyst.
- Type III (Calcified/Dead cysts): Thesecysts show echogenic calcifications on ultrasound, which are characterized by posterior shadowing. On CT, they are hyperattenuating, and on MRI, they appear hypointense.
- Type IV (Complicatedcysts): Complications of hydatid cysts may arise from rupture due to degeneration, intervention, trauma, or superimposed infection. In cases of contained rupture, floating membranes can beobserved as serpentine structures with low attenuation on CT and low signal on MRI, commonly referred to as the 'Water-lilysign'. The presence of intra-cystic air mayindicate a communicating rupture and/or super infection.
- An abdominal ultrasoundis a systematic procedure with sensitivity rates ranging from 93% to 97%. This imaging technique is particularly effective for detecting hydatid cysts, which predominantly localize in the liver, while also allowing for the evaluation of other abdominal sites [6,10]. In the case under discussion, the liver appeared normal.
- Al though the mortality rate associated with echinococcosis is relatively low, the condition can result in significant disabilities. The prognosisis contingent upon the specific type of infestation.
Morbidityprimarily arises from the rupture or infection of cysts, as well as dysfunctions of the affectedorgans, which may include cirrhosis, biliary obstruction, and bronchial obstruction, among others.
The reported mortality rate associated with this condition ranges from 0.29% to 0.6%. This mortality is primarily attributable to factors such as anaphylaxis, systemic complications (including sepsis and respiratory failure), or the variable characteristics of the infection. These factors can depend on several keyvariables: (a) the specificorgan affected, (b) the size and location of the cyst, (c) the interactions between enlargingcysts and sur rounding organs, and (d) complications arisingfromcyst rupture [11- 13]. In the case of our patient, the prognosiswas particularly poor due to the severe localization of the condition and itsproximity to the cardiaccavities, whichled to a potentialpre-tamponade situation.
Effective treatmentis contingent upon early detection and comprehensive surgical excision. The surgical strategy is determined by the cyst'sspecific location and the involvement of adjacent structures [6].
The effectiveness of albendazole as a medical treatment continues to be a topic of discussion among health care professionals. This medicationis commonly prescribed in the postoperative phase, particularly for patients demonstrating indications of disease dissemination or those with ruptured cysts [5]. Additional scenarios warranting its use include inoperable primary cysts in the liver or lungs, cysts located at multiple sites, and peritoneal cysts [14]. Considering these factors, we proposed an albendazole-based treatment regimen for our patient following a collaborative discussion, especially in light of the patient'sunwillingness to proceed with surgical intervention.
This highlights the unfavorable prognosis experienced by our patient, attributable to the delayed diagnosis, which occurred at a late stage. Additionally, the patient's refusal of surgery further contributed to the unfortunate outcome, ultimately resulting in her demise.
Conclusion
This case study illustrates the remarkable correlation between a pulmonary hydatidcyst and pulmonary embolism, resulting in diastolic restriction and pulmonary hypertension. Despite the ongoing prevalence of hydatid disease in variousregions, its unusual presentations— particularly those involving cardiac structures—pose considerable diagnostic and therapeutic challenges. The compressive impact of the cyst on cardiac chambers resulted in significant hemodynamic implications, ultimately leading to a pre-tamponade state. Prompt diagnosis and timely intervention are paramount in averting complications and enhancing patient outcomes. Although surgical excision is regarded as the standard treatment for large hydatidcysts, situations involving patient refusal or delayed presentation may require the use of medical therapy with albendazole, which can exhibit variable efficacy. This case emphasizes the necessity for heightened clinical vigilance, particularly in endemicregions, to ensure the swift identification and effective management of complex presentations of hydatiddisease.
Funding:
The authors declare that no funding was received for this study
Ethics, Consent To Participate, And Consent To Publish:
Ethical approval was not required for this case report. Written informed consent was obtained from the patient (or the patient’s legal guardian) for participation and publication.
Clinical Trial Number:
Not applicable.
Ethics Approval:
This study was approved by the Ibn Rochd University Hospital ethics committee.
Informed consent was obtainedfrom the patient and her family.
Data Availability Statement:
The data of this study are available from the authors upon reasonable request.
References
- R. Morar and C. Feldman, “Pulmonary echinococcosis,” European Respiratory Journal, vol. 21, no. 6, pp. 1069–1077, 2003.
View at Publisher | View at Google Scholar - Pedrosa I, Saíz A, Arrazola J, Ferreirós J, Pedrosa CS. Hydatiddisease: radiologic and pathologic features and complications. Radiographics 2000;20(3):795–817.
View at Publisher | View at Google Scholar - O ˘guzkaya F, Akçali Y, Kahraman C, Emiro ˘gullari N, Bilgin M, Sahin A. Unusually located hydatidcysts: intrathoracic but extrapulmonary. Ann ThoracSurg 1997;64(2):334–7.
View at Publisher | View at Google Scholar - T. Pakala, M. Molina, and G. Y. Wu, “Hepaticechinococcalcysts: areview,” Journal of Clinical and Translational Hepatology, vol. 4, no. 1, pp. 39–46, 2016.
View at Publisher | View at Google Scholar - Traibi A, Atoini F, Zidane A, et al. Mediastinal Hydatid. Cyst J Chin Med Assoc 2010; 73:3-7.
View at Publisher | View at Google Scholar - Eroğlu A, Kürkçüoğlu C, Karaoğlanoğlu N, et al. Primaryhydatidcysts of the mediastinum. Eur J Cardiothorac Surg 2002; 22:599-601.
View at Publisher | View at Google Scholar - Saeedan MB, Aljohani IM, Alghofaily KA, LoutfiS, Ghosh S. Thoracichydatid disease: A radiologicreview of unusual cases. World J Clin Cases 2020;8(7):1203–12. doi: 10.12998/wjcc. v8.i7.1203
View at Publisher | View at Google Scholar - Mohammadi A, Khodabakhsh M. Multiple mediastinalhydaticcysts: a case report. TuberkToraks 2011; 59:70-2.
View at Publisher | View at Google Scholar - Goenka AH, Das CJ, Goel P, et al. Giant primary posterior mediastinal hydatid cyst in a child: report of a case and review of literature. PediatrSurg Int 2009; 25:647-9.
View at Publisher | View at Google Scholar - Ozpolat B, Ozeren M, Soyal T, et al. Unusuallylocatedintrathoracicextrapulmonarymediastinalhyd atidcystmanifesting as Pancoast syndrome. J ThoracCardiovascSurg 2005; 129:688-9.
View at Publisher | View at Google Scholar - Parija SJ. Textbook of medicalparasitology. 2nd ed. All India Publishers and Distributors; 2004 [chapter 11], p. 221–29.
View at Publisher | View at Google Scholar - Kokakusak A, Koyuncu A, Arikan S, Senturk Q. Primaryhydatidcyst of vastislateralis muscle. Acta Chir Belg 2004; 104:471–2.
View at Publisher | View at Google Scholar - Arora V, Nijjar IS, Gill KS, Singh G. Case report: primaryhydatidcyst of muscle – a rare site. Indian J Radiol Imaging 2006;16(2):239–41.
View at Publisher | View at Google Scholar - Manterola C, Otzen T, Muñoz G, Alanis M, Kruuse E, Figueroa G. Surgery for hepatichidatidosis. Risk factors and variables associatedwithpostoperativemorbidity. Overview of the existingevidence. Cirugía de la hidatidosishepática. Factores de riesgo y variables asociadas al desarrollo de morbilidadpostoperatoria. Revisión global de la evidenciaexistente. Cir Esp 2017;95(10):566–76. doi: 10.1016/j.ciresp.2017.08.009
View at Publisher | View at Google Scholar
