

Case Report | DOI: https://doi.org/10.31579/2835-8295/124
A Tale of Two Culprits: A Rare Case Report
1Department of Cardiology, Christian Medical College, Vellore, Tamil Nadu, India.
2First Author: Dr Shobhit Priyanshu Joseph Department of Cardiology, Christian Medical College, Vellore, Tamil Nadu, India.
*Corresponding Author: Amit Mandal, Department of Cardiology, Christian Medical College, Vellore, Tamil Nadu, India.
Citation: Amit Mandal, Shobhit Priyanshu Joseph, Senthilnathan P, (2025), A Tale of Two Culprits: A Rare Case Report, International Journal of Clinical Reports and Studies, 4(3); DOI:10.31579/2835-8295/124
Copyright: © 2025, Amit Mandal. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 05 May 2025 | Accepted: 13 June 2025 | Published: 27 June 2025
Keywords: acutest elevation myocardial infarction; cardiogenic shock; percutaneous coronary intervention; double culprit vessel occlusion
Abstract
Acute ST elevation myocardial infarction is frequently because of occlusion of single culprit vessel. The occurrence of acute thrombotic occlusion in multiple coronary arteries leading to STEMI is a rare observation in coronary angiography during primary angioplasty for myocardial infarction (PAMI). Double culprit vessel occlusion in acute STEMI is infrequent and accompanied by cardiogenic shock and ventricular arrythmias and sudden cardiac death. Prompt restoration of normal coronary flow can salvage the myocardium and decrease a possible risk of death from complications. We reported a case involving a 66-year-old male who experienced an acute infero-postero-lateral STEMI accompanied by cardiogenic shock and ventricular arrythmias. Coronary angiography revealed thrombotic occlusions in both the right coronary artery (RCA) and circumflex arteries. The patient's clinical condition improved only after undergoing percutaneous transluminal coronary angioplasty (PTCA) on both arteries. Due to the uniqueness of this presentation, there is no standardized management approach. Additional studies are necessary to enhance outcome predictions and inform future treatment strategies.
Introduction
Double culprit vessel occlusion is rare in patients presenting with ST-segment elevation myocardial infarction (STEMI). Clinical presentation can be complicated by cardiogenic shock, ventricular arrythmias or sudden cardiac death (SCD). The mechanism is most probably related to vulnerable coronary plaques. (1-4) We presented the case of a man with acute infero-postero-lateral STEMI caused by thrombosis of two major coronary arteries complicated by cardiogenic shock and ventricular arrythmias.
Case Description
A 66-year-old gentleman with comorbidities of type 2 diabetes mellitus and hypertension was transferred to our department with acute STEMI, 3 hours of window period in killip class IV and runs of NSVT. On admission, the patient was having active chest pain with perspiration. His heart rate was regulary irregular with 106 beats/min, blood pressure 84/56 mm Hg, and saturation 96% without oxygen. Physical examination revealed fine rales over the basal lung fields. ECG showed ST elevation in II III aVF, V5-V6, V7-V9, reciprocal ST depression in V1-V3 with VPC’s (Figure 1). He was taken up for primary PCI reperfusion strategy and coronary angiogram revealed a thrombotic occlusion of major obtuse marginal (OM) artery the branch of left circumflex (LCX) artery and thrombotic occlusion of mid to distal segment of right coronary artery (RCA). (Figure 2).
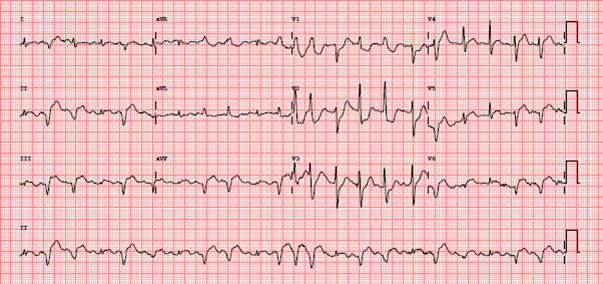
Figure 1. Initial ECG showed ST elevation in II III aVF V5-V6, horizontal ST depression V1-V3, VPC’s
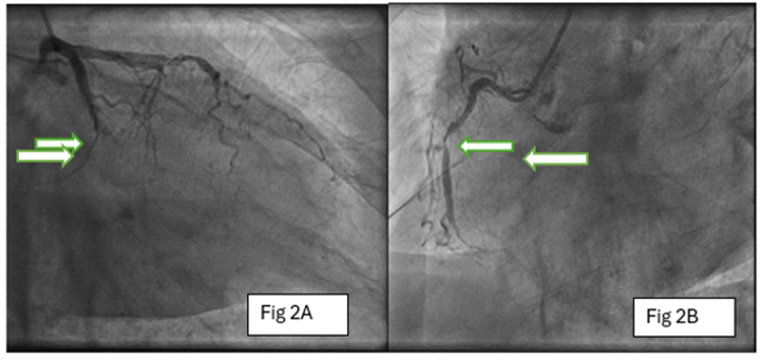
Figure 2. Angiogram showed thrombotic occlusion of both (A) LCX-OM and (B)mid-distal RCA (Double culprit vessels) (White arrow)
LCX- Left circumflex OM- Obtuse marginal RCA- Right coronary artery
As the visible thrombus was seen in LCX-OM branch pre-dilatation and deployment of a 2.75× 33 mm (Xience Prime, Abbot) drug-eluting stent (DES) was done. There was no change in patient’s symptoms – angina and further had a VT during procedure for which 150J DC cardioversion was done and ST elevation still persisted. Hence, it was decided to stent the RCA lesion also. Mid-distal RCA into the RPDA 2.75x48mm (Yukon choice, Translumina), proximal to mid RCA 3x48mm (Yukon choice, Translumina) and ostial RCA 3.5x15mm (Xience Prime, Abbot) drug-eluting stent were deployed. TIMI 3 flow restored (Figure 3) in the RCA. At this stage, the clinical condition and hemodynamic state of the patient significantly improved.
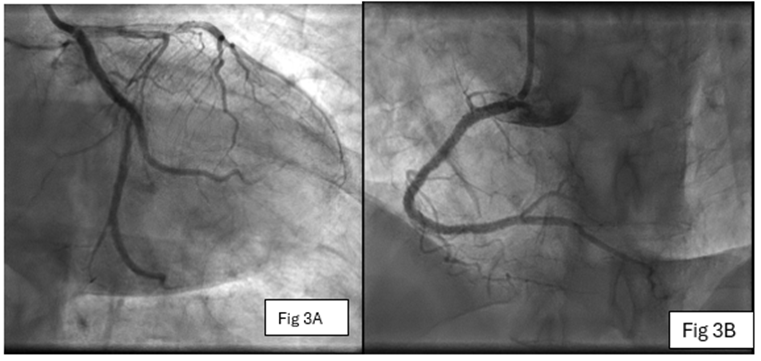
Figure 3. Post PPCI good TIMI III flow down the vessels (A) LCX-OM and (B) RCA
PPCI - Primary percutaneous intervention
LCX- Left circumflex OM- Obtuse marginal RCA- Right coronary artery
After the procedure, ECG showed normal sinus rhythm and good ST resolution (Figure 4). Echocardiography revealed mild left ventricular systolic dysfunction with ejection fraction of 46% with no mechanical complications. On day four, the patient was discharged in good medical condition without signs of congestive heart failure (CHF).
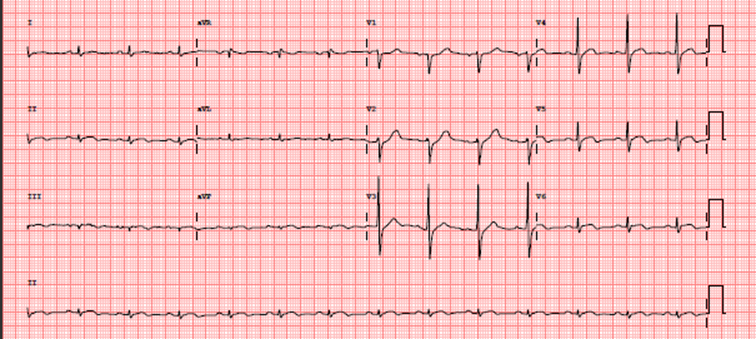
Figure 4. Post PPCI ECG showed resolution of ST elevation in II III aVF V5-V6
PPCI - Primary percutaneous intervention
ECG - Electrocardiogram
Discussion
The main mechanism of acute STEMI is the rupture of the vulnerable coronary plaque with subsequent thrombus formation and vessel occlusion. [1] Usually, it is recognized by a single-culprit lesion; however, in rare cases, multivessel coronary artery occlusion may occur at the same time in patients with acute MI. [2,3] Most patients with double coronary artery occlusion may present with cardiogenic shock, acute pulmonary edema, malignant arrythmias or SCD. [4] The mechanism of multivessel coronary artery thrombosis remains unclear but different contributing factors could be suggested such as a hypercoagulable state, cocaine use, or an essential thrombocytosis. [2] None of these factors were present in our patient; however, he was elderly with type 2 diabetes mellitus and hypertension and denied any addictions. In acute MI, inflammation of the pancoronary vessels may occur predisposing to plaque instability and thrombosis in multivessel coronary arteries. [5]
Our patient was admitted with acute infero-postero-lateral STEMI, complicated by cardiogenic shock and ventricular arrythmias. We managed the above complications with single inotropic support with injection noradrenaline infusion for cardiogenic shock and DC cardioversion and amiodarone for ventricular arrythmias. In the case of cardiogenic shock due to acute STEMI, myocardial revascularization is the only evidence-based therapy with proven survival benefit. [6,7] Considering all those options, we concluded that for our patient the best choice is primary PCI. Coronary angiography revealed occlusion of LCX-OM artery and mid to distal RCA. ECG finding on admission was suggestive more of LCX as culprit vessel. So, due to a visible thrombus in LCX-OM artery, it was first decided to open this artery with restoration of TIMI 3 flow. However, patient's condition did not improve, and he had a VT during procedure for which 150J DC cardioversion was done and ST elevation still persisted. Hence, it was decided to stent the RCA lesion also. After the TIMI III flow in both occluded coronary arteries, the clinical and hemodynamic condition of our patient was significantly improved. Prompt intervention in both occluded coronary arteries and restoration of normal coronary flow was the best therapy for this patient, myocardium was salvaged, and possible risk of death from complications was decreased.
Conclusion
An unusual variant of STEMI involving multi-vessel coronary thrombosis is associated with a high rate of cardiac complications. Our case highlights a STEMI with two culprit vessels, where clinical outcomes significantly improved following the primary angioplasty (PAMI) procedure on both vessels. Therefore, we strongly advocate for performing percutaneous transluminal coronary angioplasty (PTCA) on both culprit vessels during the same session, especially if the initial culprit vessel shows no improvement after the first PCI procedure.
Ethics approval: The patient's son provided written informed consent to be published as a case report.
Acknowledgments: Thanks to the patient and his family for the informed consent
Competing interests: No conflict of interest is to be declared by the authors.
Funding: This study received no external funding
References
- Goldstein JA, Demetriou D, Grines C, et al. (2000). Multiple complex coronary plaques in patients with acute myocardial infarction. N Engl J Med.; 343:915-922.
View at Publisher | View at Google Scholar - Kanei Y, Janardhanan R, Fox JT, Gowga RM. (2009). Multivessel coronary artery thrombosis: literature review. J Invasive Cardiol.;21(3):66-68.
View at Publisher | View at Google Scholar - Feng G, Dongnan H, Tianran D. (2012). Acute multivessel coronary artery occlusion: a case report. BMC Res Notes.;5(1):523.
View at Publisher | View at Google Scholar - Araszkiewicz A, Olasinska-Wisniewska A, Skorupski W, Lesiak M, Mularek-Kubzdela T, Grajek S. (2009). Simultaneous occlusion of 2 coronary arteries – a rare cause of cardiogenic shock. Am J Emerg Med;27(9): 1175.e5-7.
View at Publisher | View at Google Scholar - Asakura M, Ueda Y, Yamaguchi O, et al. (2001). Extensive development of vulnerable plaque as a pan-coronary process in patients with myocardial infarction: an angioscopic study. J Am Coll Cardiol.; 37:1284-1288.
View at Publisher | View at Google Scholar - Neumann F, Sousa-Uva M, Ahlsson A, et al. (2018). ESC/EACTS
View at Publisher | View at Google Scholar - Guidelines on myocardial revascularization The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J. 2019; 40:87-165.
View at Publisher | View at Google Scholar - Ibanez B, James S, Agewall S, et al. (2017) ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J.; 39:119-177.
View at Publisher | View at Google Scholar
