

Review | DOI: https://doi.org/10.31579/2834-8745/021
A Retrospective Study of Outcome in Omalizumab Therapy in Chronic Urticaria, a Real Experience on 36 Kuwaiti Patients from a Single Tertiary Dermatology Center
1Lecturer of Dermatology, Venereology and Andrology, Faculty of Medicine,Menoufia University Egypt
2Specialist of dermatology; As’ad Al-Hamad Dermatology Center Kuwait.
*Corresponding Author: Iman Almasry, Lecturer of Dermatology, Venereology and Andrology, Faculty of Medicine, Menoufia University Egypt.
Citation: Iman Almasry, Viktor Lazarevic, Nadia Alnaki, Ghadeer Alaawi, Ali Sadek, Atlal Allfai, (2024), A Retrospective Study of Outcome in Omalizumab Therapy in Chronic Urticaria, a Real Experience on 36 Kuwaiti Patients from a Single Tertiary Dermatology Center. Journal of Scientific Research and Biomedical Informatics 3(4); DOI:10.31579/2834-8745/021
Copyright: © 2024 Iman Almasry, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 July 2024 | Accepted: 19 July 2024 | Published: 26 July 2024
Keywords: patients; healthcare system; Chronic urticaria.
Abstract
Chronic urticaria (CU) is a common skin disease, characterized with wheals and itching, with or without angioedema. It is inflicting a substantial burden for patients, their family, and friends, the healthcare system,and society Chronic urticaria impacts -quality of life more than coronary artery disease or respiratory allergy.
First line of the therapy are antihistamines. However,H1-antihistamine treatment leads to absenceof symptoms in fewer than 50% of patients. Up-dosing of second-generation H1-antihistamines (up to fourfold) as recommended by the urticaria guideline, as second-line therapy can improve response; however, many cases do not respondto antihistamines and need a more effectiveapproach Second line would be to increasethe dose of antihistamines, above the licensed doses, is frequently required and still leaves a substantial proportion of patients symptomatic.
Hence, short-term corticosteroid therapy (3–7 days) may be required. Unfortunately, for most unresponsive CU patients’ longer periods of corticosteroid therapy are needed and are associated with numerous undesired side effects.
Introduction
Chronic urticaria (CU) is a common skin disease, characterized with wheals and itching, with or without angioedema. [1-3] It is inflicting a substantial burden for patients, their family, and friends, the healthcare system, and society Chronic urticaria impacts -quality of life more than coronary artery disease or respiratory allergy. [4,5] First line of the therapy are antihistamines. However, H1- antihistamine treatment leads to absence of symptoms in fewer than 50% of patients. Up-dosing of second- generation H1-antihistamines (up to fourfold) as recommended by the urticaria guideline, as second-line therapy can improve response [6]; however, many cases do not respond to antihistamines and need a more effective approach. [1,7,8,]
Second line would be to increase the dose of antihistamines, above the licensed doses, is frequently required and still leaves a substantial proportion of patients symptomatic. [1-3]
Hence, short-term corticosteroid therapy (3–7 days) may be required. Unfortunately, for most unresponsive CU patients’ longer periods of corticosteroid therapy are needed and are associated with numerous undesiredside effects. [1-4]
Refractory disease requires further interventions, third line, using cyclosporine A, omalizumab, or montelukast. Low dose cyclosporine A is efficacious in 70% of patients with glucocorticoid-dependent CSU; however, this response generally
lasts in only 50% of responders.[5] Furthermore, toxicity associated with cyclosporine A therapy, although less common following the use of low doses as required for CU, still raises concern.
The discovery of IgE by Professors Kimi Shige and Teruko Ishizaka has had a significant effect on the diagnosis and management of allergic diseases. About 40 years later, a monoclonal anti- IgE antibody, omalizumab, has been developed and opened a new era against various severe allergic diseases.[9] Omalizumab, a monoclonal antibody against immunoglobulin E (IgE) isrecommended as add- on treatment in adults and adolescents (≥12 years) with CU. That is the first drug approved for use in patients with CSU who remain symptomatic despite H1-antihistamine treatment. Omalizumab binds to free IgE, which lowers free IgE levels and results in subsequent downregulation of the FcεRI on basophils and mast cells.[8]
Definite mechanism of action is still not recognized, but there are few theories, including: reducing the capacityof mast cell to release mediators, impact on basophils and eosinophils, reducing activity of IgE autoantibodies, and decreasing coagulation abnormalities associated with disease activity.[9,10] Recent studies showed that omalizumab may intervene in immune mediated processes throughdirect basophil stabilization,[11] effects on pathogenic IgE antibodies [12], or a decrease in IgE synthesis by targeting membrane IgE-positive B cells.[13]
Omalizumab dosing for moderate-severe asthma is based on IgE levels and body weight. The effect of omalizumab on CU seems to be unrelated to these parameters.[13] Moreover, even a single injection was found to be beneficial in some of patients, as noted also in other observational and small clinical studies. [14,15] In contrast, in phase III studiesof omalizumab for CU a fixed dose of 300 mg/month was the most efficacious. [15,16]
In the study by Maurer et al., [7], the proportion of patients completely free of hiveswas 10%, 23% and 53%, in those receiving placebo, 150 mg omalizumab, and 300 mg omalizumab, respectively. In another study, even higher doses of 450 mg/month were needed for some patients. [8]
CU is a disease of spontaneous remission and exacerbation; thus, the length of therapy with Omalizumab or other immune modulators is yet to be determined. In the randomized clinical studies published so far, recurrence of symptoms followingtermination of 3– 6 months therapy was common. [8,9,11]
Omalizumab treatment show rapid response, although there is individual variability; reduces the use of oral corticosteroids and immunosuppressants; improves quality of life of the patients with CU. [11,12]
Treatment with Omalizumab is well tolerated, some patient can experience flare up of their urticaria after first or secondinjection of Omalizumab.[13] Autologous serum skin test (ASST)-positive patients were more likely to show a slow response to omalizumab therapy. Non- responders tend to have lower baseline total IgE levels, higher proportions of elevated IgG-anti- thyroid peroxidase (TPO), higher ratios of IgG-anti-TPO to total IgE and shorter treatment periods. [14,15] Patients with higher baseline total IgE levels and longer disease durations are more likelyto experience rapidrelapse after discontinuation of omalizumab. However, Omalizumab treatment was an effective therapy option. [14,15]. Omalizumab is effective and safe therapy option for patients with CU. [16,17] A Joint initiative by The European Academy of Allergy and Clinical Immunology (EAACI), the European Union-funded network of excellence, the Global Allergy and Asthma European network (GA2LEN), the European dermatology forum (EDF) and the World Allergy Organization (WAO), has provided a thorough and systematic guidelines for classification and treatment of urticaria in 2006, updated in 2009. [17,18].
Plan of the study
In winter 2014 our urticaria subspecialty clinic (Urticaria clinic, as ‘ad Al-HamadDermatology Center Kuwait)
cwas established for patients with chronic urticaria in order to standardize the treatment and diagnostic work- up in our OPD (outpatient department), the protocol of clinic has been based on the guidelines of the EAACI/GA2LEN/EDF/WAO. [17,18]
All patient's demographic data, previous treatments and paraclinical values for all referred patients from either dermatologists or general practitioners in the primary health care center. Our management with Omalizumab was started according to GA2LEN/EDF/WAO guidelines. [17,18]
Our study included all patients who have been regularly follow up in C.U.C since inception of our urticaria clinic until December 30, 2020. Patientswho lost follow up were excluded, Omalizumab was staredfor patients who were not controlled on full doses of antihistamines in addition to other previously given treatments e.g., systemic steroids. The treatment was not protocolized, so not all
paraclinical values were statically analyzed in our patients, and a modification from the describedtreatment algorithm depended on the clinical history and the social life or work situations of studied patients.
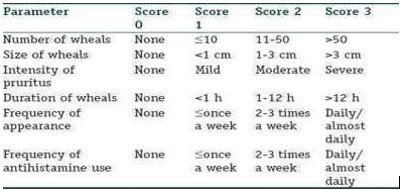
The registered CIU patients’ information’s was collected from their archived files, all available information including the age, sex, the total treatment time in our outpatient clinic, and the effect of Omalizumab treatment, were recorded along with blood biochemical tests, including C.B.C, LF, RF, TFT, antinuclear antibodies, CRP, and hepatitis serology, total and specific IgE. The Omalizumab dosage, frequency of injection, effect and total duration of therapy was alsorecorded. The effect ofOmalizumab was divided into no effect, a partial remission and complete remission; this was based purely on the subjective classification of the patient. Through medical and past history or psychic trauma,family history of CIU, and associations with angioedema were registered. Urticaria severity score was calculated into, U. SCORE 0 (basic score) before starting omalizumab, then at week 4 of treatment.…. Till week 16, table 1. A partial effect, in which the patient felt some improvement of their symptoms but not sufficient enough get back to their everyday routines was recorded (for our patients 50% reductions in number of wheals, and a subjective improvement in symptoms).
For4months as minimum duration for controlling CIU with completeremission on Omalizumab alone was estimated, for patients who had2020 not been controlled after 4 months, a combined treatment has been added
End date for studywas 30th June 2020, so totalduration of Omalizumab patients were on, was not calculated beyond that date. The data was analyzed using descriptivestatistics, using t-test and chi square testing.
Table 1. Calculation of total urticariaseverity score.
Results
The total number of patients was 36; 10 males and 25 Females. The minimum age was 7 year and maximum were 65 years with mean age 40.31. The minimum duration of urticaria was 2months and maximum 312 months with median duration 12 months, the Omalizumab treatment total duration minimum was 40 and maximum 72 with mean 48.11. There were 29 (80.5%) patients who controlled with complete remission of urticaria on omalizumab therapy alone, while 2(5.5%) controlled on combined omalizumab with cyclosporine. There were 4 (11.1%) on omalizumab combinedwith dapsone and one patient (2.2 %) on omalizumab with azathioprine. Omalizumab dosage schedule was as follow, 31 patients were on 300mg every 4 weeks, two patients were on Omalizumab 450mg every 4 weeks as they were not controlled on 300mg every 4 weeks, while three patients were on 300mg every3weeks.Two children a brother and sister were maintained on 150mg every aged 7 and 12 years consecutively.
All studied patient did not have any family history of chronic urticaria except two patients, a brother and sister of 7, 12 years consecutively. Five patients had history of psychic traumaor major depressedmood related to onset of urticaria as one female patienthad developed urticaria because her son had major cardio surgery, the other four because of undefined life stress. Thyroid functions and anti-thyroid antibodies were normal except in 3 patients who have shown high anti thyroid antibodies as the anti- thioperoxides antibodies was significant high.
Other allergic disorders, 6 patients had bronchial asthma, one of them also had allergic rhinitis, one patient was known to have penicillin allergy. Other autoimmune disorders 6 patients had hypothyroidism on replacement hormonal therapy.Screening for infection in patients were negative, only one female patient has significant pyuria, and one has vaginal candidiasis and another patient has H. pylori. A female patient had history of pemphigoid gestationis, who developed also chronic urticaria few months after resolution of pemphigoid gestationis. Antinuclear antibody (ANA), and, C-reactive protein (CRP) titers were within normal with a little high value of both markers for three patients only. Total IgE level was with in normal except for three patient had shown high values ,800,1683 and 1799 KUA/L, however six patients patients had high specific IgE , ,two have shown allergy to house dust mites (D.petronys ,D.fariance ,Siro Mites,Purterscentiae) mites, other two for Cat dander, animals, cockroach insects, prosopis and last two for
plant pollen and sea food(shrimp fish…..). One patient had urticaria after given meningoencephalitis vaccine before the Haj pilgrimage. All patients who were adherent on regular Omalizumab injection, but 5 patients who discontinued treatment after complete remission, had relapse aftervariable times ranging from afew months to 2 or 3 years, and those who were restartedon treatment, were fully controlled again. Another two patients had a relapse during regular treatment without discontinuation Omalizumab because of undefined cause, and another one patienthad relapse after receiving blood transfusion, and another patient with relapse with from an unknown cause.
The Statistical correlations of studied patientshad shown a non-significant relation between Urticaria severity score (USAW-0) and total durationof urticarial as P value 0. 947 table 3. Correlation between urticaria severity score (USAW-0) and remissions duration was non- significant table 4. Regard treatment there was a non- significant correlation between U. SCORE 0 and treatment, P value was.133 table 5. Correlation between duration of Omalizumab therapy (in months) and urticaria Severity score U. SCORE 0 was non-significant P value.108 table 6.
Table (2) Demographic data and treatments of studie presented as number and % exceptfor the duration.
| Patients’ variables | No. | % |
| Sex Total | 36 | 100 |
| Female | 26 | 72.2 |
| Male | 10 | 27.8 |
| Age (years) | ||
| minimum - maximum | 7-65 | |
| Mean+SD | 40.31+12.70 | |
| Duratio | ||
| n U(months) | ||
| Minimum - maximum | 2- 312 | |
| Median (IQR) | 12(86) | |
| Duration.Omal. (months) | ||
| minimum - maximum | 40-70 | |
| Mean+SD | 48.11+6.99 | |
Treatment | ||
| Omalzimumab | ||
| Omal. +Cyclosporine. | 29 | 80.5 |
| Omal. +Dapson | 2 | 5.5 |
| Omal. +Immuran | 4 | 11.1 |
| 1 | 2.7 | |
Table3.Correlation between U. SOR0 and Urticaria Duration
| U. SCORE 0 | Mild | Moderate | Severe |
| N | 10 | 15 | 11 |
| Minimum | 3 | 3 | 2 |
| Maximum | 96 | 312 | 240 |
| Q1 | 3.75 | 6.00 | 4.000 |
| Median | 5.50 | 36.00 | 24.00 |
Q3 | 24.00 |
96.00 |
121.00 |
| Spearman'srho | |||
| Correlations | _012 | ||
| Correlation Coefficient | |||
| P value |
.947 |
Remissions by duration(weeks) | Urticaria score0 |
LL-χ2(2) |
P-value | ||||
Mild | Moderat e |
Severe |
Total | ||||
USAW4 | No | 9 | 15 | 11 | 35 |
2.637 |
0.267 |
Yes |
1 |
0 |
0 |
1 | |||
USAW8 | No | 3 | 9 | 9 | 21 |
6.063 |
0.048 |
Yes |
7 |
6 |
2 |
15 | |||
USAW1
2 | No | 1 | 4 | 3 | 8 |
1.349 |
0.509 |
Yes |
9 |
11 |
8 |
28 | |||
USAW1
6 | No | 0 | 0 | 1 | 1 |
2.437 |
0.296 |
Yes |
10 |
15 |
10 |
35 | |||
Table 4: Correlation between urticaria severity score (USAW-0) and Remissions duration.
Remissions by duration(weeks) | Urticaria score0 |
LL-χ2(2) |
P-value | ||||
Mild | Moderat e |
Severe |
Total | ||||
USAW4 | No | 9 | 15 | 11 | 35 |
2.637 |
0.267 |
Yes |
1 |
0 |
0 |
1 | |||
USAW8 | No | 3 | 9 | 9 | 21 |
6.063 |
0.048 |
Yes |
7 |
6 |
2 |
15 | |||
USAW1
2 | No | 1 | 4 | 3 | 8 |
1.349 |
0.509 |
Yes |
9 |
11 |
8 |
28 | |||
USAW1
6 | No | 0 | 0 | 1 | 1 |
2.437 |
0.296 |
Yes |
10 |
15 |
10 |
35 | |||
Table 5. Correlation betweenU. SCORE 0 and treatments.
| Treatments | U. SCORE 0 | |||
| Mild | Moderate | Severe | Total | |
Omalizumab |
7 |
14 |
8 |
29 |
| Omal.+ Cycl. | 1 | 1 | 0 | 2 |
| Omal. + Da. | 1 | 0 | 3 | 4 |
| Omal. +Az. | 1 | 0 | 0 | 1 |
Total |
10 |
15 |
11 |
36 |
| Chi-Square | 9.799 | |||
| Likelihood Ratio | ||||
| Df | 6 | |||
| P value | 0.133 | |||
UCSORE0 |
Omalizumab therapy (in months) | ||||
N |
Mean |
SD |
Minimum |
Maximum | |
| Mild | 10 | 44.70 | 3.65 | 42.0 | 54.0 |
| Moderate | 15 | 50.67 | 8.27 | 43.0 | 72.0 |
| Severe | 11 | 47.73 | 6.45 | 40.0 | 60.0 |
| Total | 36 | 48.11 | 6.99 | 40.0 | 72.0 |
| F-value | 2.385 | ||||
| p | 0.108 Not significant | ||||
Table 6. Correlation between duration of Omalizumab therapy (in months) according to urticaria Severity score U. SCORE 0
Discussion
Chronic spontaneous urticaria is a challenge both for the patient and the physician. First of all, its name (CSU) gives some idea on its perplexity, there is no real cause, nor immunopathogenesis, and as its name suggests it tends to be recurrent\ chronic and comes on spontaneously without prior warning.
It might seem to be a trivial disease, but in reality, it can be severe and socially distressing and have a major impact on the quality of life these patients. In addition, relapsing course which made it is comparable with patients who have severe coronary artery disease24. Unsuccessful control of chronic spontaneous urticaria despite up-dosing to fourfold of antihistamines as large number of patients up to a third to fourth patient will remain symptomatic. [25] Hence alternative treatments are needed for poorly controlled, Omalizumab is the appropriate therapy, for this group of patients, Omalizumab has been approved by international guidelines, for patients who do not respond to higher-dose H1 antihistamine therapy. [26] Omalizumab is a humanized IgG1k monoclonal antibody that specifically binds to free human IgE, which was firstly indicated for the treatment of allergy-induced asthma. [27]. In 2014, FDA approved Omalizumab for patients affected by CSU aged 12 years or older who continue to have symptoms.
In our study Omalizumab dosage schedule was used accordingto EAACI/GA2LEN/EDF/WAO treatment guidelines algorithm, but not in protocolized manner, rather by discretion. Chronic urticaria duration of our studied patients was maximum 312 months (26year)and minimum 2 months, the U.SCOR0 was not affected by long durationof urticaria as P value = 0. 947 table. 3. All studied patients were not controlled either on full dose, antihistamines, intermittent course of oral or injectable steroids, neither montelukast, (leukotrienes antagonists).
There is no significant correlation between UCSORE0 nor with remission duration table.4. There is non-significant correlation between the given treatments whatever Omalizumab alone or combined with cyclosporine, dapson or azthioprine with U.SCOR0 table.5 , although previous studies have been shown rapid urticaria resolution with cyclosporine, dapson and tacrolimus. [26,28,29]
The studied patients who were not controlled on omalizumab alone for 16 weeks and, a combined treatment was added (cyclosporine, dapson, azathioprine) but the combined treatments did not show anyadditional improvements regardless urticaria score severity as no significant correlation is found, P value=.133 that table5.
The dosage schedule for Omalizumab Injection was changed either to be given at a shorter durationof every two, orthree weeks, or increasing the dose of Omalizumab dose to450mg, depending on the patient’spreference for patients were not controlled on 300mg every week, the up dosing of Omalizumab to 450mg was reported by Fiorino et al. [30] Omalizumab had shown complete clinical control of urticaria, regardless duration, severity, as a non-significant relation of U. SCOR0 with Omalizumab therapy total duration table.6. Most studied patients had not been kept adherent on regular antihistamines with an individual variability of regimen regarding frequency of dosing, t y p e of antihistamine (sedating or non- sedating) or even complete discontinuation of antihistamines, but all experienced improved life quality.
The studied patients were included two children who put on 150 mg every 4 weeks, a written consent taken from their parents to give Omalizumab as it is an off- label treatment in pediatric34, after failureof controlling urticaria by antihistamines and systemic steroids. Safety and effectiveness of omalizumab in pediatric was reported in a study done by Coco Dekkers, et al. [34] No. ne of our patients had experienced any serious adverse reactions, 7 patients (19.4%) had site injection pain, 3 patients had mild transient headaches (8.3%), one (2.7 %) patient experienced epistaxis (The patient was reassured and was referred to Ear,Nose & Throat)for management), to our knowledge this is an unknown side effect to Omalizumab. These findings show that Omalizumab is well tolerated with no serious adverse reactions in chronic urticaria patients. [35]. Omalizumab is the only approved add-on treatment for CSU patients aged 12 years or older who do not respondto H1 antihistamines in both Europe and the US [36]
A different dosage schedules were used in different publications include up dosing of Omalizumab. [37,38,30]
Omalizumab is effective therapyfor chronic urticaria, which licensed dose of 300 mg in Europe and either 150mg or 300mg in the USA by subcutaneous injectionevery 4 weeks. [31]
Some reports have shown examples of the optimization of omalizumab treatment in patients who show inadequate response by increasing the dose or decreasing the dosing intervals.[32]
Our study had the flexibility of being able to increase the dose or decreasethe dosing intervals, in treatment regimen rather than a constant regimen interval.
This was done for the aim to gain full controlof the patient’s symptoms, and this was on par with is previous published studies. [32,33] Omalizumab is well tolerated, a relatively safe drug, with minimal adverse reactions like injection site reaction, and very rarely serious ones as, anaphylaxis
which has been reported in 0.09% of patients with allergic asthma. [39,40]. All paraclinical values were done for our studied patients, and they were mostly normal,this was also shown in previous studies [41], and no clinical significance of these values were found in omalizumab therapy protocol for chronic urticaria in our studied patients.
So therefore, extensive tests are not needed for chronic urticaria patients, only in exceptional cases in which history may support further investigations. Patients of chronic urticaria can be put on different dosage schedules, or combined treatments lines.
Conclusion
Chronic urticaria is an autoimmune skin disease in which most investigations including, blood chemistry, infection screening, Multiple-antigen simultaneous test (MAST) specific IgE antibodies, or total IgE are mostly normal.
Omalizumab is considered a good controlling therapy in non-responders to antihistamines for chronic urticaria. The continuation of Omalizumab injection is needed as maintenance c.ontrol of urticaria.
References
- Ioana Agache, Claudio Rocha,Ana Pereira, Yang Song, Pablo Alonso-Coello, Ivan Solà, Jessica Beltran, Margarita Posso, at all. (2020), Efficacy and safety of treatment with omalizumab for chronic spontaneous urticaria: A systematic review for the EAACI Biologicals Guidelines. GUIDELINES. DOI: 10.1111/all.14547.
View at Publisher | View at Google Scholar - Eyerich S, Metz M, Bossios A, Eyerich K. (2020), New biological treatments for asthma and skin allergies. Allergy; 75(3):546-560.
View at Publisher | View at Google Scholar - Maurer M, Abuzakouk M, Bérard F, et al. (2017), The burden of chronic spontaneous urticaria is substantial : real-world evidence from ASSURE- CSU. Allergy; 72:2005-2016.
View at Publisher | View at Google Scholar - O'Donnell BF, Lawlor F, Simpson J, Morgan M, Greaves MW. (1997), The impact of chronic urticaria on the quality of life. Br J Dermatol; 136:197-201.
View at Publisher | View at Google Scholar - Baiardini I, Giardini A, Pasquali M, et al. (2003), Quality of life and patients' satisfaction in chronic urticaria and respiratory allergy. Allergy; 58:621- 623.
View at Publisher | View at Google Scholar - Schoepke N, Asero R, Ellrich A, et al. (2019), Biomarkers and clinical characteristics of autoimmune chronic spontaneous urticaria: Results of the PURIST Study. Allergy; 74(12):2427-2436.
View at Publisher | View at Google Scholar - Maurer M, Raap U, Staubach P, et al. (2019), Antihistamine-resistant chronic spontaneous urticaria : 1-year data from the AWARE study. Clin Exp Allergy; 49:655-662.
View at Publisher | View at Google Scholar - Metz M, Ohanyan T, Church MK, Maurer M. (2014), Omalizumab is an effective and rapidly acting therapy in difficult-to-trea.t chronic urticaria: a retrospective clinical analysis. J Dermatol Sci; 73(1): 57-62.
View at Publisher | View at Google Scholar - Maggi L, Rossettini B, Montaini G, et al. (2018), Omalizumab dampens type 2 inflammation in a group of long-term treated asthma patients and detaches IgE from FcεRI. Eur J Immunol.;48(12):2005-2014.
View at Publisher | View at Google Scholar - Yoshimichi Okayama, Hisako Matsumoto, Hiroshi Odajima, Shunsuke Takahagi, Michihiro Hide, Kimihiro Okubo. (2020), Roles of omalizumab in various allergic diseases. Allergology International 69, 167-77.
View at Publisher | View at Google Scholar - Kaplan AP, Giménez-Arnau AM, Saini SS. (2017), Mechanisms of action that contribute to efficacy of omalizumab in chronic spontaneous urticaria. Allergy ;72(4):519-533.
View at Publisher | View at Google Scholar - Gericke J, Metz M, Ohanyan T, et al. (2017), Serum autoreactivity predicts time to response to omalizumab therapy in chronic spontaneous urticaria. J Allergy Clin Immunol.; 139:1059-1061.
View at Publisher | View at Google Scholar - Metz M, Maurer M. (2012), Omalizumab in chronic urticaria. Curr Opin Allergy Clin Immunol; 12: 406- 11.
View at Publisher | View at Google Scholar - Chan MA, Gigliotti NM, Dotson AL, Rosenwasser LJ. (2013), Omalizumab may decrease IgE synthesis by targeting membrane IgE+ human B cells. Clin Transl Allergy; 3 (1): 29.
View at Publisher | View at Google Scholar - Marzano AV, Genovese G, Casazza G, Fierro MT, Dapavo P, Crimi N, Ferrucci S, Pepe P, Liberati S, Pigatto PD, Offidani A, Martina E, Girolomoni G, Rovaris M, Foti C, Stingeni L, Cristaudo A, Canonica GW, Nettis E, Asero R. (2019), Predictors of response to omalizumab and relapse in chronic spontaneous urticaria: a study of 470 patients. J Eur Acad Dermatol Venereol. May;33(5):918-924. doi: 10.1111/jdv.15350. Epub 2018 Dec 7. PMID:30451325.
View at Publisher | View at Google Scholar - Sussman G, Hébert J, Barron C, et al. (2014), Real- life experiences with omalizumab for the treatment of chronic urticaria. Ann Allergy Asthma Immunol; 112 (2): 170-4.
View at Publisher | View at Google Scholar - Yudi Chena, Miao Yub, Xiaojie Huang, Ping Tub, Peikun Shig, Marcus Maurerh and Zuotao Zhaob. (2021), Omalizumab treatment and outcomes in Chinese patients with chronic spontaneous urticaria, chronic inducible urticaria, or both. World Allergy Organization Journal 14:100501.http://doi.org/10.1016/j.waojou.2020.10 0501
View at Publisher | View at Google Scholar - Jariwala SP, Moday H, de Asis ML, Fodeman J, Hudes G, de Vos G, Rosenstreich D.(2009),Ann Allergy Asthma Immunol. Jun;102(6):475-82.
View at Publisher | View at Google Scholar - Maurer M, Weller K, Bindslev-Jensen C, et al. (2011), Unmet clinical needs in chronic spontaneous urticaria. A GA2LEN task force report. Allergy;66: 317–30.
View at Publisher | View at Google Scholar - Zuberbier T, Aberer W, Asero R, Bindslev-Jensen C, Brzoza Z, Canonica GW, et al. (2014), The EAACI/GA LEN/EDF/WAO Guideline for the definition, classification, diagnosis, and management of urticaria: the 2013 revision and update. Allergy. [PubMed] [Google Scholar]
View at Publisher | View at Google Scholar - Tedeschi A, Contini M, Asero R. (2009), Simultaneous occurrence of chronic autoimmune urticaria and non-allergic asthma: a common mechanism? Eur Ann Allergy Clin Immunol. 41:56.
View at Publisher | View at Google Scholar - Doong JC, Chichester K, Oliver ET, Schwartz LB, Saini SS. (2017), Chronic idiopathic urticaria: systemic complaints and their relationship with disease and immune measures. J Allergy Clin Immunol Pract.5(5):1314–8.
View at Publisher | View at Google Scholar - Grob JJ, Revuz J, Ortonne JP, Auquier P, Lorette G. (2005), Comparative study of the impact of chronic urticaria, psoriasis and atopic dermatitis on the quality of life. Br J Dermatol; 152:289-295.
View at Publisher | View at Google Scholar - O’Donnell BF, Lawlor F, Simpson J, Morgan M, Greaves MW. The impact of chronic urticaria on the quality of life. Br J Dermatol. 1997; 136:197–201. [PubMed] [Google Scholar]
View at Publisher | View at Google Scholar - Maurer M, Weller K, Bindslev-Jensen C, Giménez- Arnau A, Bousquet PJ, Bousquet J, et al. (2011), Unmet clinical needs in chronic spontaneous urticaria. AGA2LEN task force report. Allergy Eur J Allergy Clin Immunol. 66:317–30.
View at Publisher | View at Google Scholar - Zuberbier T, Aberer W, Asero R, et al. (2018), The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and management of urticaria. Allergy; 73:1393.
View at Publisher | View at Google Scholar - Global initiative for asthma. Global strategy for asthma management and prevention; 2017Available from: www.ginasthma.com. Accessed August 09, 2019.
View at Publisher | View at Google Scholar - Booth SA, Moody CE, Dahl MV, et al. (1992), Dapsone suppresses integrin-mediated neutrophil adherence function. J Invest Dermatol; 98:135.
View at Publisher | View at Google Scholar - Seth S, Khan DA. (2017), The Comparative Safety of Multiple Alternative Agents in Refractory Chronic Urticaria Patients. J Allergy Clin Immunol Pract; 5:165.
View at Publisher | View at Google Scholar - Fiorino I, Loconte F, Rucco AS, Nico A, Vacca M, Damiani E, Nettis E, Caiaffa MF, Macchia L (2014) Long-term treatment of refractory severe chronic urticaria by omalizumab: analysis of two cases. Postepy Dermatol Alergol 31(5):332–334. https://doi.org/10. 5114/pdia.2014.44023
View at Publisher | View at Google Scholar - FDA U (2014) Xolair® (omalizumab) for injection, for subcutaneous
View at Publisher | View at Google Scholar - Turk M, Kocaturk E, Cure K et al (2018) Two-week intervals during omalizumab treatment may provide better symptom control in selected patients with chronic urticaria. J Allergy Clin Immunol Pract 6(4):1389–1390.
View at Publisher | View at Google Scholar - Larenas-Linnemann DES, Parisi CAS, Ritchie C, Cardona-Villa R,Cherrez-Ojeda I, Cherrez A, Ensina
View at Publisher | View at Google Scholar - LF, Garcia E, Medina IV,Rodríguez-González M, Caraballo JMS (2018) Update onomalizumab for urticaria: what’s new in the literature from mechanisms to clinic. Curr Allergy Asthma Rep 18(5):33. https://doi.org10.1007/s11882-018-0787-5.
View at Publisher | View at Google Scholar - Coco Dekkers, Mehran Alizadeh Aghdam, Marlies de Graaf, André C Knulst, Yolanda Meijer 2, Juul M P A van den Reek, Marike B Stadermann, Heike Röckmann (2021) Safety and effectiveness of omalizumab for the treatment of chronic urticaria in pediatric patients, Multicenter Study Pediatr Allergy Immunol May;32(4):720-726.
View at Publisher | View at Google Scholar - Francés L, Leiva-Salinas M, Silvestre J. (2014), Omalizumab in the treatment of chronic urticaria. Actas Dermosifiliogr; 105:45-52.
View at Publisher | View at Google Scholar - Vestergaard C, Toubi E, Maurer M, et al, (2017), Treatment of chronic spontaneous urticaria with an inadequate response to H1-antihistamines: an expert opinion. Eur J Dermatol; 27:10-9.Rottem M, Segal R, Kivity S, et al: (2014),
View at Publisher | View at Google Scholar
