

Review Article | DOI: https://doi.org/10.31579/2835-7957/035
The Role of The Multidisciplinary Team
- Rehan Haider *
Riggs Pharmaceuticals Karachi Department of Pharmacy, University of Karachi-Pakistan.
*Corresponding Author: Rehan Haider, Riggs Pharmaceuticals Karachi Department of Pharmacy, University of Karachi-Pakistan.
Citation: Rehan Haider. (2023), The Role of The Multidisciplinary Team, Clinical Reviews and Case Reports, 2(4); DOI:10.31579/2835-7957/035
Copyright: © 2023, Rehan Haider. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 05 June 2023 | Accepted: 13 June 2023 | Published: 19 June 2023
Keywords: patient outcomes, barrier challenges, integration technology, artificial intelligence, decision-making, case studies, healthcare settings, community health centers
Abstract
The role of multidisciplinary crews is an essential part of the modern healthcare structure. This study aimed to explore and elucidate the importance of multidisciplinary teams (MDTs) in numerous healthcare settings, including hospitals, clinics, and network health centers. MDTs contain experts from various disciplines, including but not confined to physicians, nurses, psychologists, social workers, pharmacists, and therapists, who collaboratively work together to offer comprehensive and holistic affected person care. This paper will delve into the advantages of MDTs, emphasizing how they foster effective communication, enhance patient consequences, and enhance overall satisfaction with care. Furthermore, it will study the challenges and obstacles that MDTs may encounter, including variations in professional perspectives and capacity conversation gaps. Techniques for overcoming these challenges may also be discussed, focusing on the significance of establishing clean protocols and inspiring mutual recognition among team contributors. Additionally, the function of leadership within MDTs can be highlighted, as powerful leadership is instrumental in guiding the crew toward un unusual dreams. This paper will discover the features of successful MDT leaders and their capability to foster a collaborative and supportive environment. Case studies and real-life examples of MDTs in motion may be provided to illustrate their sensible software and effect on patient care. Furthermore, the paper discusses the ability to integrate generation and artificial intelligence into MDTs, inspecting how these advancements can further optimize teamwork and decision-making procedures.
Introduction
According to the World Health Organization (WHO), four chronic non-communicable diseases (diabetes, cancer, and respiratory and cardiovascular diseases (CVD)account for 60% of global deaths (i.e., 35 million deaths per year) [1]. In Europe and China, 30 – 40% of patients with acute myocardial infarction have a known history of diabetes. In the remaining subjects, 70% of patients have either diabetes or intermediate hyperglycemia on formal 75-g oral glucose tolerance testing [2, 3]. In addition, diabetes and hypertension frequently co-exist. Both are important in the majority of cardiovascular deaths worldwide, which are estimated to be 18 million annually. The number of people with diabetes is projected to increase from 285 million in 2010 to 435 million by 2030 [4]. The resulting increase will lead to considerable losses in productivity and greatly increase the burden on the healthcare system. The treatment of diabetes and its associated complications is costly. In 2006, the WHO estimated that 2.5–15% of healthcare budgets were spent on diabetes-related illnesses in developing and developed areas. The International Diabetes Federation (IDF) estimated that 7–13% of the annual healthcare expenditure is spent on the treatment of diabetic complications [5]. The total direct annual cost of diabetes in eight European countries is estimated at € 29 billion, with an estimated yearly cost of € 2834 per patient [6]. In the USA, diabetes is associated with annual direct medical expenditures direct medical expenditures of $91.8 billion. The per capita cost was estimated at $13,243 for individuals with diabetes compared to $2560 for those without diabetes [7]. In China, one of the countries with the fastest increase in diabetes prevalence, $558 billion in national income is expected to be lost over the next 10 years owing to premature deaths caused by non-communicable diseases, including heart disease, stroke, and diabetes [8]. Early diagnosis and aggressive control of risk factors can prevent complications in both type 1 (T1DM) and type 2 diabetes mellitus (T2DM) [9–11] International organizations, such as the IDF, as well as many national organizations, have published clinical recommendations and set standards to guide clinical practice, optimize metabolic control, and prevent complications [12].
Evidence for the optimization of diabetes control
To date, most evidence supporting the beneficial effects of optimal diabetes care on clinical outcomes [10,13,14] has been collected under closely supervised clinical trial conditions. In the Diabetes and Complications Clinical Trial (DCCT), which lasted for 6.5 years, patients with T1DM treated intensively had an HbA 1c level 2% (22 mmol/mol) lower than those who were conventionally (7.2% vs. 9.1%, 55 vs. 76 mmol/mol). After the study was completed, the authors continued to follow these patients in the Epidemiology of Diabetes Interventions and Complications (EDIC) Study. There was progressive deterioration in glycemic control once these intensively treated patients returned to their usual care setting; however, patients previously treated conventionally also improved, and both groups converged to achieve HbA 1c levels 8% (64 mmol/mol) [15]. Despite this convergence, patients previously treated intensively maintained over 50% risk reduction in all diabetes-associated complications, including cardiovascular events [16]. Similar findings have also been reported in the UK Prospective Diabetes Study (UKPDS). People with T2DM who were previously treated with an intensive regimen continued to have lower rates of complications and all-cause mortality than patients treated conventionally 10 years after discontinuation of the trial [17]. In the Steno - 2 Study, individuals were treated in an attempt to attain control for all major risk factors (HbA 1c, blood pressure [BP], and low-density lipoprotein [LDL] cholesterol), it had a 50 – 60% risk reduction in microvascular and macro vascular complications compared with those conventionally treated [18]. As in the DCCT and UKPDS, in the post-Steno study period, people who had been treated intensively in the main trial maintained more than 60% risk reduction in all-cause death compared with those conventionally treated for 13.3 years [19]. Findings from these landmark studies demonstrated the beneficial effects of achieving risk factor control during the early course of the disease to achieve long-term benefits.
Diabetes care: the Reality
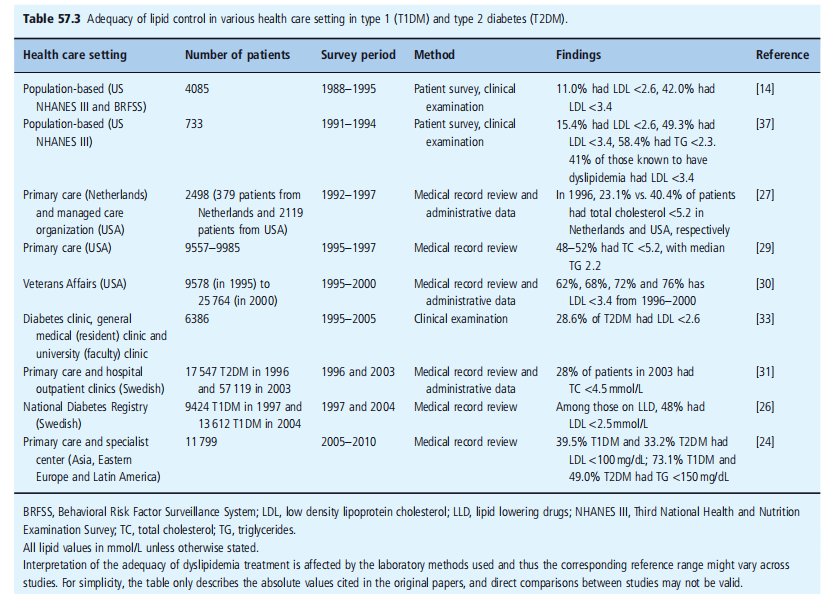
Regardless of the evidence, extensive and international surveys have indicated that diabetes manipulation remains suboptimal for a large number of the studied populations and fitness care settings. It should It ought to additionally be remembered that most of the people of these recommendations, guidelines, surveys, and research emanate from settings, countries, and particularly well-resourced areas. in line with the country-wide health and dietary exam Surveys (NHANES), done between 1988 – 1994 and 1999 2002 in the USA, amongst sufferers with diabetes elderly 18–74, Even though there has been a non-giant bargain in the proportion of patients with HbA 1c > 9% (> seventy-five mmol/mol), because the number of sufferers with HbA 1c 6–8% (64–86 mmol/mol) advanced, there has been no sizeable trade-in implying HbA 1c among those intervals [20]. In the 1999 – 2002 survey, there was accelerated use of multiple antidiabetic marketers for management [21], yet almost half of them had HbA 1c tiers greater than the American Diabetes Association (ADA) recommendation, with 7% and 20% having HbA 1c > 9% (> 75 mmol/mol). There was also no significant opportunity in the distribution of blood pressure, with 33% having BP > 140/ninety mmHg. From the 1999 – 2002 survey, 60% executed LDL cholesterol concentrations of < 3>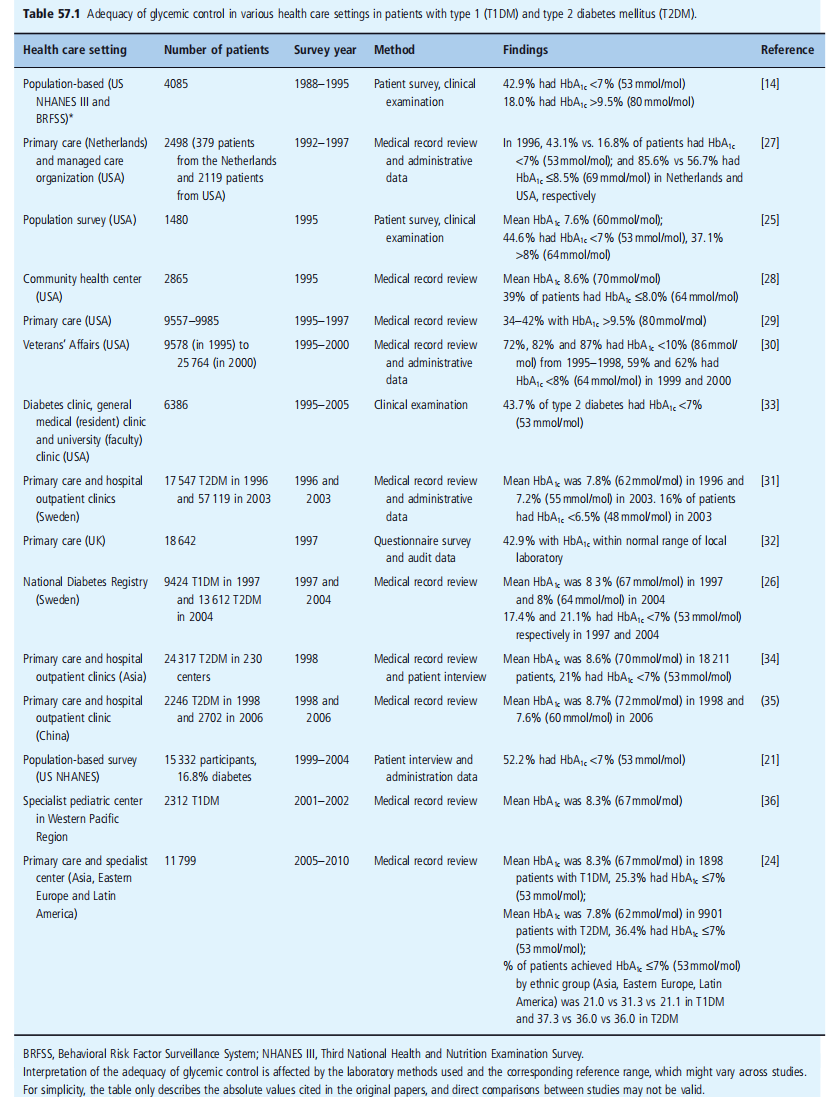
T2DM could achieve target systolic and diastolic blood pressures of ≤ 140 and ≤ 90 mmHg, respectively [34]. Emerging evidence of the importance of blood pressure control has led to the revision of the target blood pressure to < 130>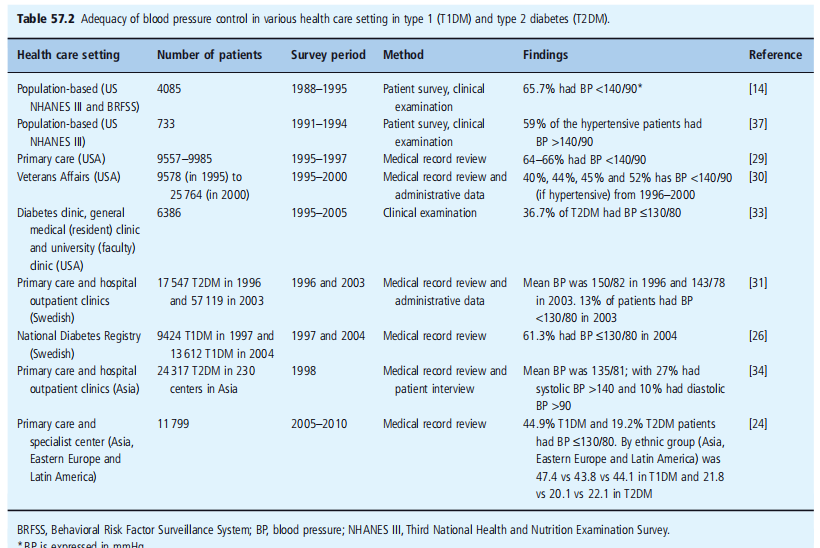
There was a slow but gradual improvement in lipid control (Table 57.3), probably because of the effective treatment of LDL cholesterol with 3-hydroxy-3- 3 - methyl - glutaryl - coenzyme A (HMG-CoA) reductase inhibitors. In the 1980s and the early 1990s, the rate of achievement of target LDL cholesterol < 2>
Approximately 25–30% [24,27,29,31,33]. For HMG-CoA reductase inhibitors, as illustrated by a study In Sweden, nearly half of the patients were able to achieve the target [26].
There are obvious limitations to these studies, including the heterogeneity of populations in different studies, retrospective reviews, incomplete documentation for medical record review, and accuracy of claim data. Despite the limitations and lack of comparability of the many studies, the results summarized in Tables 57.1–57.3 indicate the same trend. It should also be noted that Most of these surveys come from well-resourced settings and developed countries, where laboratory assessments of HbA 1c are readily available.
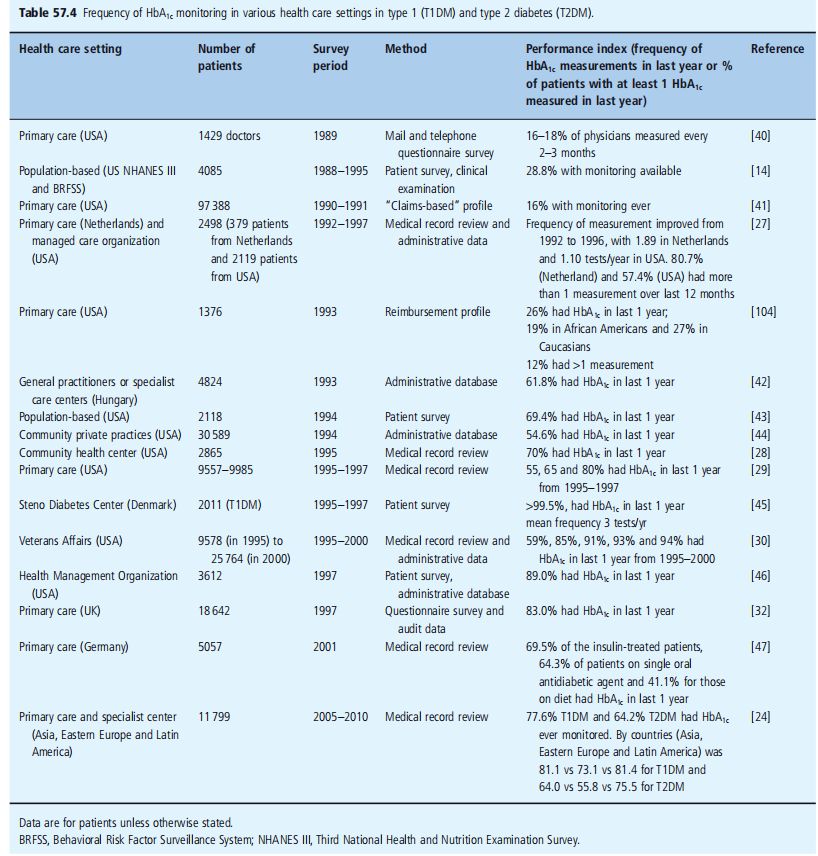
The Institute of Medicine defines quality of care as “the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge [38, 39]. There is an ongoing controversy as to the degree to which outcomes can be directly related to processes of care, yet both are considered important measures of quality; thus, the degree of adherence to recommended guidelines, based on available clinical evidence, guides the degree of quality of care. Table 57.4 summarizes attempts to address this specific issue and includes surveys that assess the quality of care as measured by the frequency of measurement for HbA 1c. In the early years, less than one-third of the 1990s, with the availability of results from the DCCT and UKPDS, the frequency of monitoring gradually improved [27, 29, 42, 44]. More than 90% of patients have HbA 1c regularly monitored in specialist clinics such as the Steno Diabetes Center [45] and in some primary care settings [30, 46]. Monitoring is available for 70–80% of patients [24, 32, 47]. It is important to note that there is often a discrepancy between doctors’ claims of the frequency of monitoring and that occurring in practice. Although there appear to have been some improvements in the care processes over time, this has not been matched by an improvement in the rates of achieving treatment targets (Tables (57.1–57.3).
The discrepancy between evidence-based and reality the efficacy of optimization of diabetes control has been found in randomized controlled trials conducted with stringent clinical trial protocols; however, despite improvements in some processes of care, such as monitoring of HbA 1c, this has not been matched by an improvement in the rates of achieving treatment targets. In addition, the level of care received by many patients does not meet the recommended standards. In a previous survey in the USA, only 25% of the patients were aware of the term “glycated hemoglobin.” or “HbA 1c” [43]. Only 72% of participants visited the healthcare facility. provider for diabetes care at least once a year, and approximately 60% underwent complication screening. Furthermore, despite the proven benefits of many therapeutic agents, many people with diabetes are not prescribed insulin, angiotensin-converting enzyme (ACE) inhibitors, or lipid-lowering drugs despite the presence of indications [48 – 53]. The factors that compromise the quality of care have been examined in various studies but are not well understood. Nevertheless, some components were evident. Patients Drug compliance by patients receiving chronic medications is consistently reported as being less than 50%, often because of insufficient education and reinforcement [54–56] Moreover, there is Considerable heterogeneity in the patterns and rates of non-adherence to individual components (e.g., diet, exercise, and drugs) of a diabetes treatment regimen. Thus, the extent to which people
In diabetes, adherence to one aspect of the regimen might not correlate with adherence to other components. Previous studies have shown that only 69% of people with diabetes follow a diet and less than half of them engaged in regular exercise [57]. The reported adherence to self-monitoring of blood glucose ranges from 53% to 70% [58]. Earlier studies have indicated that only 7% of patients with diabetes adhere to all aspects of the treatment regimen [59], while over half made errors with insulin dosage, and three-quarters of patients were judged to be in an “unacceptable”
category regarding the quality, quantity, and timing of meals [60]. In attempts to extrapolate results from clinical trials to daily practice, it is important to individualize interventions, taking into account all potential factors. For example, on the elderly, side the effects of interventions must be balanced against their long-term benefits, limited life expectancy, and comorbidities. Other factors such as education level, access to care, compliance, and motivation may also contribute to patient adherence, in addition to treatment-related factors such as adverse effects, polypharmacy, and costs [42, 43, 49]. It is recommended that people with diabetes should be educated about the nature of the disease, with a particular focus on chronicity and long-term complications, as well as preventing the ability
Physicians
The key role of healthcare providers is to equip people with diabetes with knowledge and skills related to self-management, individualize medical and behavioral regimens, assist with informed
decisions, and provide social and emotional support via collaborative relationships [61, 62]. An important factor is the inertia of physicians in failing to modify the management of patients in
response to abnormal clinical results [63, 64]. In a previous study, according to Kaiser Permanent, one of the major health management organizations in the USA, there were, on average, 15 and 21 months of lapse before the escalation of treatment in patients with HbA 1c > 8% (64 mmol/mol) on metformin and sulfonylurea monotherapy, respectively [65]. Despite the complexity and rapid advances in diabetes management, generalists often do not perceive a need for further training in the field of diabetes [66–69]. The involvement of other non-medical healthcare professionals may not be welcomed in some traditional settings.
Health care system
Traditional medical practice is organized to respond quickly to acute problems but does not adequately serve the need. HbA1c 7% (53 mmol/mol) and LDL cholesterol < 2>
In this survey, there was considerable heterogeneity between regions of patient-related factors (e.g., age, disease duration, presence of complications, body weight), health care systems (e.g., health insurance coverage, availability of specialist care, training by diabetes educators), and self-care (e.g., self-adjustment of insulin). dosage) were associated with the likelihood of reaching targets. The problem is particularly marked in low and middle-income settings where it is exacerbated by multiple demands upon severely limited resources, including those imposed by a continuing burden of infectious diseases and other issues, such as accidents and injuries
The evolving concept of d disease management
It is clear from the preceding sections that even though gold standard care improves medical results in medical trial settings, it is frequently not executed in real scientific situations for the reasons discussed. This has led to attempts to develop methods of care based on multidisciplinary processes. In recent years, there has been a growing emphasis on control through the coordination and organization of the personal components of care rights into devices. The latter is further supported using reinforcement via multiple contacts, including not only doctor appointments, but also smartphone reminders and visits to other healthcare professionals, including nurse practitioners, dietitians, and pharmacists. In step with Wagner et al. [70], there are five key factors to improve the effects of sufferers with persistent disease:
1 A gadget to assist with using evidence-based pointers
2 Reorganizations of practice structures and crew features
3 affected persons self-management assistance;
4 improved access to expertise and availability of medical facts to facilitate monitoring and feedback on doctors’ overall performance.
5 The Steno-2 look affords top-notch proof in the guide of
The benefits of protocol-driven multifaceted care include the use of a multi-disciplinary approach for T2DM [13, 18, 19]. Patients were randomized to the in-depth remedy, and the organization was managed with the aid of a multidisciplinary team according to a protocol that specified a stepwise implementation of conduct modification, smoking cessation, competitive manipulation of glycemia, BP, lipids, and micro albuminuria, and the use of an ACE inhibitor and aspirin. The reductions in HbA1c,
BP, serum cholesterol and triglycerides levels, and albuminuria had been all significantly extra within the intensive care organization than in the same old care institution. these benefits in metabolic manipulation have been translated to threat reductions of cardiovascular morbidity and
mortality by 53% (95% confidence interval [CI] 27–76%), nephropathy by 71% (95% CI, 1383%), retinopathy with the aid of 58% (95% CI 14–79%), and autonomic neuropathy by 63% (95% CI 21–82%). By way of the stoop of 13.3 years, sufferers previously treated intensively had lower all-cause mortality (hazard ratio [HR]). 54; 95% CI 0.32 – 0.89), cardiovascular events (HR 0.43; 95% CI 0.19 – 0.94), and cardiovascular occasions (HR 0. 41; 95% CI 0.25 – 0.67) than the traditional care group.
In any other multicenter randomized study evaluating strike-through care added by way of a Diabetologist–nurse group with conventional care, 60% of patients with T2DM with renal impairment receiving established care attained three or more predefined need treatment dreams (HbA 1c < 7>
or more had a 60% threat reduction in all-cause mortality and stop-level renal disease (HR 0.43; 95% CI 0.21) 0.86) [71].
Implementation of quality standards Care
This concept of disease management emphasizes an organized, proactive multidisciplinary approach to health care in complex and chronic diseases, of which diabetes is a prime example
[72,73]. Individuals with chronic diseases should be empowered to improve their knowledge and self-management [74, 75]. Preferences should be considered when individualizing treatment plans.
Evidence suggests that periodic attendance at a diabetes center [76] and frequent reminders by paramedical staff to reinforce self-management could improve metabolic control, clinical outcomes, and survival [13, 71, 77–84]. Clinical information should be readily available to provide support. Information technology can be used to monitor adherence to guidelines and provide feedback to care providers (see Chapter 58) [70, 72, 85–87]. The provision of structured care to individuals with T2DM is best implemented through a series of interlinked processes based on these principles. These include risk stratification, protocol-driven care, regular review by a multidisciplinary team, patient empowerment, and good record-keeping to monitor progress (Figure 57.1
Risk stratification
Diabetes is characterized by the clustering of a couple of threat elements that engage in a complicated way to give rise to a couple of headaches [88]. every member of the IDF and American Diabetes Association (ADA) recommends that humans with diabetes go through a complete assessment at presentation and yearly thereafter to record nonpublic, medical, and laboratory measurements. This permits stratification of risk and placement of patients in unique care plans for
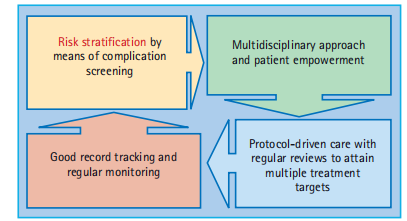
Figure 57.1 Components for quality structured care.
focused and individualized treatment. The UKPDS has provided longitudinal statistics which enable outlining the herbal statistics of cardiovascular complications in T2DM. Using the UKPDS information, mathematical models were evolved to pick out predictors (hazard factors) for cardiovascular ailment [89]. in addition, the Framingham heart examination started in 1948, has prospectively observed a big organization of individuals in the general populace to perceive elements contributing to the development of CVD, and danger engines have additionally been superior to waiting for the hazard of CVD in this population [90]. each the UKPDS and the Framingham threat equations show mild effectiveness in hazard stratification in the UK and US settings; however, outside validation research shows that the general performance varies extensively among international locations and ethnic businesses [91]. Similarly, there had been only a few hundred human beings with diabetes inside the genuine cohort of Framingham, at the same time as the UKPDS recruited individuals within the early section of diabetes. These pose precise obstacles in utilizing the hazard engines derived from those two studies to trendy diabetes populations in Europe, the US, and elsewhere. Further, amendment and development of ethnic-particular threat equations have now been carried out. for instance, equations to anticipating diabetes headaches including coronary heart ailment, stroke, stop-degree renal failure, and congestive coronary heart failure, similar to average mortality, have now been developed for the Chinese language populations based on prospective compliance with-up of approximately 8,000 patients, with an average look-at-up of 6 years [89, 92–95]. on this unique enterprise of Chinese-language humans with diabetes, the Framing Ham's stroke threat engine underestimates, while the UKPDS engine overestimates the danger of stroke. both of the threat engines for CVD overestimate the threat of CVD in a few populations, together with the Chinese language. in addition, it became no longer viable to broaden the UKPDS threat engine to evaluate the chance of end-degree renal disorder as in addition, development in this area is predicted with the enlargement of studies into one-of-a-type settings and ethnicity-unique areas.
Protocol-driven organizations are using a multidisciplinary approach Diabetes management involves multiple contacts with different healthcare personnel, each specializing in a particular process or area of expertise. Non-medical personnel, notably nurse educators, nutritionists, pharmacists, physical trainers, and podiatrists are key members of a successful diabetes team. While doctors adopt the leading and coordinating role in defining problems and needs, the professional knowledge and clinical skills of these non-medical staff are invaluable in providing counseling and holistic care for patients. These healthcare professionals can also assist physicians in providing follow-up, empowering self-management, and helping caregivers of patients with cognitive impairment and bodily disabilities. This group method permits physicians to spend extra time in the dialogue of wishes, setting goals and alternatives in the control group. For high-hazard individuals, which include those with comorbidities or those receiving a couple of medicinal drugs, the pharmacist may have a unique position in offering training to patients in collaboration with physicians to enhance the secure and powerful use of pharmaceutical sellers and reduce the risk of drug-related unfavorable outcomes and drug-drug interactions. Given the large number of processes and employees probably concerned with the shipping of such evidence-based and protocol-pushed care, it is crucial to try to determine which elements of care can be attributed to which components. In a meta-analysis of 66 publications analyzing 11 special strategies to enhance diabetes care [96], two key strategies were associated with statistically significant incremental reductions in HbA1c values. The primary team adjustments, which worried about the addition of a group member, shared care between primary care and professional centers, or multidisciplinary group care, resulted in additional HbA1c. reduction using 0.33% (three.6 mmol/mol). This was related to an additional HbA1c discount of 0.22% (2. 4 mmol/mol). This finding has been replicated in numerous clinical settings. For instance, the Chinese-language College of Hong Kong Diabetes Organization has used one-of-a-kind care prototypes since the Nineteen Nineties to augment the shipping of care and usage of nurses and pharmacists. The latter became empowered to run clinics or provide phone counseling to provide periodic tests and boost compliance. These prototypes constantly showed advanced fees of treatment compliance and attainment of multiple treatment objectives, in addition to reduced hazard of dying and cardio-renal complications with the aid of 50 – 70% in continual sicknesses such as diabetes with or without complications (57. 2) [82–84]. These two techniques have emerged as key additives and are relevant globally, irrespective of healthcare placement. In much less resource-rich settings, a few of these techniques can be met, at least partly, by appropriate education or relocation of current staff in reaction to converting health needs. Patient empowerment and self-care, in addition to team changes and case management, and different approaches that have been shown to improve sickness manipulation include patient schooling (effect sizes 0.24 [0.07–0.40]), reminders (0.27 [0.17–0.36]), and economic incentives (0. 40[0.26–0.34]) [86]. At the same time, as the adherence of physicians and care providers to care techniques may additionally improve health outcomes, affected person adherence is a crucial factor in understanding the benefits of these techniques. Sufferers must actively participate in defining and achieving agreed-upon treatment dreams instead of conforming to medically described regimens or commands. In diabetes, behavioral adjustments, inclusive of adhering to a meal plan and tasty in normal physical exercise, taking medications regularly, monitoring blood Glucose levels and other complications and attending to foot care demand high levels of self-discipline and are important components of holistic care models [61]. Given the chronic nature of diabetes and the large amount of data collected during contact with care providers, there is a need to develop a system to manage this information effectively and enable healthcare workers to make decisions, track clinical progress, monitor compliance, and benchmark the quality of care. Information technology can also empower people with diabetes by making information more accessible and understandable. Such technology can also assist individuals with diabetes to keep their health records, maintain control, and use to manage their care in an informed manner (Figure 57.3}
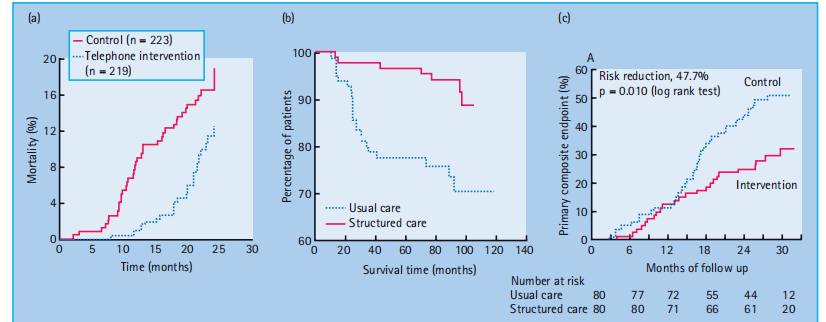
Figure 57.2 Effect of protocol - driven care using a multidisciplinary approach to reduce risk of complications in patients with chronic diseases including type 2 diabetes mellitus (T2DM) [82 – 84]. (a) Telephone counseling by a pharmacist between clinic visits reduced mortality rate by 50% in patients receiving five or more chronic medications. (b) Patients with T2DM without cardio renal complications managed in a clinical trial setting was associated with a 70% risk reduction in death rate compared with matched patients followed up in
conventional care setting. (c) Patients with T2DM with chronic kidney disease managed by a pharmacist – doctor team had a 50% risk reduction in death and end - stage renal disease compared with patients managed in conventional care setting
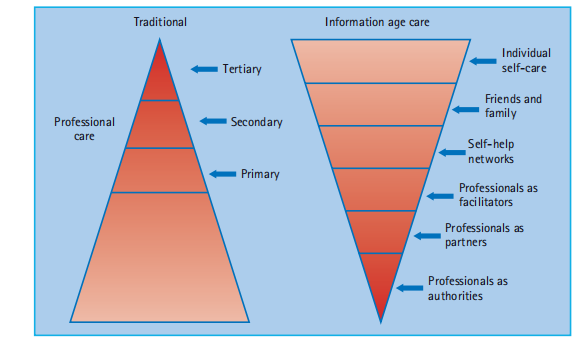
Figure 57.3 Change of paradigm using information technology to improve clinical and self - management. Adapted from Jennings et al. [109], with permission from Knowledge Exchange LLC.
Importance Of Periodic Monitoring and Review
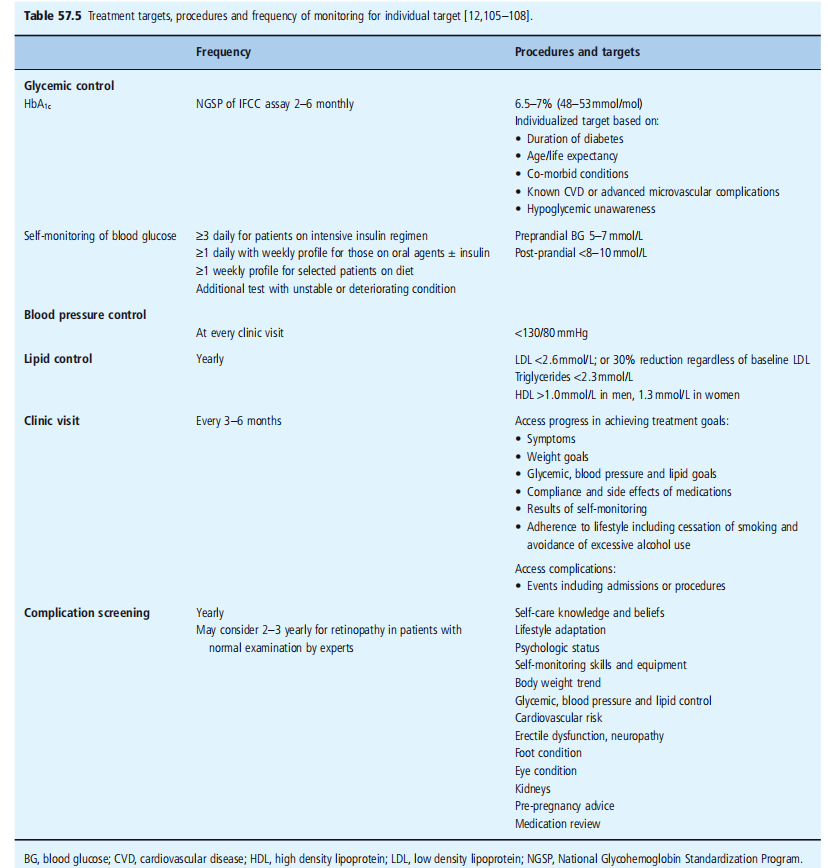
Depending on the complications and control of risk factors, people with diabetes should be reviewed at intervals ranging from weekly to every few months. However, once stabilized, people with diabetes should be reviewed by a healthcare professional at least once a year, regardless of the severity of the condition. The targets, procedures, and frequency of monitoring individual targets are summarized in Table 57.5.This takes account of the possibility of silent deterioration of metabolic control and development of new risk factors or complications, as proper management, cannot be initiated
unless control indices are measured periodically [97]. In the study shown in Figure 57.2 (a), which was conducted in the early 1990s, the omission of the measurement of metabolic
was associated with a 15-fold increase in the risk of death. The comparison group in this study had at least one measurement during the 7 years of observation [82]. These findings are related to the adjustment of regimens facilitated by periodic monitoring [97]. Patients receiving structured care have greater utilization of antihypertensive and lipid-lowering agents. Using ACE inhibitors as an example, despite compelling evidence supporting their protective effects [98], clinicians in conventional care settings often withhold or discontinue these drugs for fear of side effects such as hyperkalemia and deterioration of renal function, especially in high-risk patients who are most likely to benefit [99, 100]. This is further supported by the study shown in Figure 57.2 (c) in T2DM with nephropathy, in which 60 – 70% of patients were treated with an ACE inhibitor or ARB at baseline. At the end of a 2 - year study period, over 90% of subjects randomized to structured care delivered by a multidisciplinary team persisted with the treatment compared with less than 20% of subjects randomized to conventional care. Together with better risk factor control, increased drug usage, and more clinical and laboratory assessments, this difference in the use of ACE inhibitors or ARBs collectively contributed to the reduction in death and cardio renal event rates between the structured and conventional care groups [71, 84].
The importance of attaining multiple targets
As shown in Table 57.5, multiple treatment targets, in addition to glycemic control, need to be considered when managing people with diabetes. In an observational study of 6386
In patients with T2DM in Hong Kong, attainment of ≥ 2 treatment goals (HbA 1c, BP, or LDL cholesterol) was associated with 30 – 50% risk reduction in the new onset of CHD, demonstrating the importance of attaining multiple targets [33]. In the Steno - 2 study in Denmark, which aimed to achieve multiple risk factor control, the overall relative risk reduction of 59% in composite cardiovascular events accords with the expected cumulative effects of control of individual risk factors in an additive manner [19]. This has been further replicated in another study on individuals with diabetic nephropathy, in which more people receiving structured care attained ≥ 3 treatment goals (61%) compared to the conventional care group (28%). This difference translates to a 60 – 70% reduction in premature death and end-stage renal disease [71]. It has been estimated that the use of HMG - CoA reductase inhibitors and blood pressure-lowering drugs confer the largest benefit in reducing cardiovascular risk in the initial study period, with the optimization of glycemic control and the use of aspirin, providing additional beneficial effects. The long-term glycemic benefits–social effects of glucose-lowering on diabetes-related endpoints–are expected to occur later. Hence, the attainment of multiple treatment targets might explain the continuing divergence in cardiovascular endpoints rather than a simple time–effect relationship. The importance of sustained benefits of long-term glycemic control is further supported by the legacy effect associated with intensive blood glucose control, long after the cessation of the UKPDS [101] and the parallel findings of the DCCT/EDIC study [15,16]
Cost-effectiveness of multidisciplinary care
Cost-effectiveness analysis for intensive glycemic and blood pressure control was performed based on the results of the UKPDS [102]. The cost per quality-adjusted life year (QALY) for intensive blood glucose control with insulin or sulfonylureas was £ 6028 more than conventional treatment, whereas metformin for overweight patients costs £1021 less than conventional treatment. These estimates suggest that intensive blood glucose therapy, particularly the use of metformin in obese patients with diabetes, is effective and cost-saving. The cost per QALY gained for tight blood pressure control was £ 369 based on the UKPDS. Similarly, according to the Centers for Disease Control (CDC) in the USA, the incremental cost-effectiveness ratio for intensive glycemic control was US$41,384 per QALY.
The respective costs for intensified blood pressure control and reduction of serum cholesterol were US$1959 and US$51,889 per QALY [103]. Furthermore, these analyses suggested that these interventions were most cost-effective when instituted early in the disease course.
A similar analysis was also performed in the Steno-2 Study [19], where the incremental cost-effectiveness ratio for structured care versus conventional treatment was € 3927 and € 2538 per life-year and per QALY gained, respectively. These incremental costs were mainly attributed to the increased pharmacy and consultation costs. The author further pointed out that even assuming that patients in structured care continued to receive the most expensive treatment in a specialist setting in Denmark, and the treatment effects between the intensive and conventional groups might decline after completion of the 7.8 - year intervention period, the incremental costs still represent good value for money. However, because of the multifaceted nature of the intervention, it was difficult to identify the contribution of individual factors to improved outcomes.
1 Research method:
A randomized controlled trial (RCT) layout change was used to assess the effectiveness of a multidisciplinary care version for the control of type 2 diabetes. They looked at sufferers identified with type 2 diabetes and randomly divided them into two organizations: an intervention agency that received care via a multidisciplinary organization and a control organization that acquired widespread care
2 participants:
A total of 300 individuals with type 2 diabetes were recruited for this study. They were randomly assigned to either the intervention group (n = 150) or the control group (n = 150). Individuals in each business were matched for age, sex, duration of diabetes, and glycemic manipulation at baseline to reduce confounding factors.
3. Intervention:
The intervention institution obtained care from a multidisciplinary crew of number-one care physicians, endocrinologists, Diabetologist, registered dietitians, nurses, pharmacists, podiatrists, ophthalmologists, optometrists, intellectual health experts, exercising experts, and social employees. The group collaborated to extend individualized treatment plans, focusing on glycemic control, diet, bodily pursuits, medicine adherence, and emotional well-being.
4. Control Group:
The control enterprise received popular diabetes care, which typically protected visits to several care physicians or endocrinologists for diabetes control, with restricted involvement of different healthcare specialists.
5. Data Collection:
Baseline data, including demographic statistics, clinical statistics, and initial measures of glycemic manipulation (HbA1c levels), were accumulated for every commercial enterprise. Follow-up assessments were carried out at 3, six, and one-year durations to screen for adjustments in HbA1c tiers, blood strain, lipid profiles, frame mass index (BMI), and self-stated lifestyle measures through standardized questionnaires.
6. Result:
The results confirmed that the multidisciplinary care model had a significant impact on the diverse consequences in the assessment of standard care.
A. Glycemic control: The intervention institution showed statistically large discounts in HbA1c stages at 3, 6, and 12 months compared to the manipulated institution. This shows the development of blood sugar control in interventional institutions.
b. Blood pressure and lipid profiles: The intervention organization confirmed higher management of blood stress and lipid ranges at some unspecified time in the future, suggesting a top-notch effect on cardiovascular risk elements.
BMI and Weight management: Participants within the intervention employer established a higher BMI and weight compared to the manipulated organization, indicating the effectiveness of a multidisciplinary method in promoting a healthy way of life.
d. Quality of life Self-reported quality of life measures of satisfaction of existence, on the side of physical and emotional well-being, had been notably better within the intervention organization in comparison to the manipulated institution at follow-up.
7. Discussion:
The findings of this study will aid in the effectiveness of a multidisciplinary care approach in the management of type 2 diabetes. The collaborative efforts of multidisciplinary institutions have enabled an extra comprehensive technique of diabetes control, addressing multiple components of the state of affairs and supporting patient empowerment through education and self-control assistance.
The splendid upgrades positioned in glycemic control, blood stress, lipid profiles, BMI, and best of life within the intervention institution underscore the benefits of several healthcare specialists in diabetes care. The multidisciplinary organization model may have facilitated better medication adherence, better patient adherence to weight loss programs and lifestyle modifications, and higher psychological guidance, which are essential for fantastic health effects.
Furthermore, they take a look to highlight the significance of a patient-targeted approach to diabetes management. Customized treatment plans evolved with the aid of a multidisciplinary group to recall private alternatives, goals, and occasions, and promote patients' experiences of ownership and duty for their health.
It is vital to note that the fulfillment of a multidisciplinary care model also relies on effective verbal exchange and coordination among crew members. Ordinary meetings share digital health data, and mutual knowledge of roles and responsibilities is essential to the success of such a method.
However, they have a look and can also have a few limitations, including a noticeably quick follow-up length of 365 days, which might not seize long-term consequences. Furthermore, the generalizability of appearance may be restricted to unique healthcare settings and patient populations
Conclusions
In conclusion, T2DM is a massive public health problem associated with 10–12 years. It has major implications on quality of life, health care utilization, and
societal productivity. Diabetes management is complex, and effective management requires the creation of care models that take account of this complexity and facilitate care providers to attain multiple treatment targets and empower patients to adhere to self-management. Such models should include continuous quality improvement initiatives with the measurement of key performance indices, validated outcome measures, and risk–benefit analyses of interventions. Landmark trials such as the Steno - 2 study have demonstrated the cost-effectiveness of the use of protocol-driven multidisciplinary care to manage and prevent diabetes complications. With appropriate organization of care, good clinical governance, and patient empowerment, quality diabetes care should eventually become accessible, affordable, and sustainable.
irrespective of circumstances and resource setting
Acknowledgment
The completion of this research project would not have been possible without the
contributions and support of many individuals and organizations. We are deeply
grateful to all those who played a role in the success of this project
We also thank My Mentor [. Naweed Imam Syed Prof. Department of Cell Biology at the University of Calgary and Dr. Sadaf Ahmed Psychophysiology Lab University of Karachi for their invaluable input and support throughout this research. Their insights and expertise were instrumental in shaping the direction of this project
Declaration of Interest
I at this moment declare that:
I have no pecuniary or other personal interest, direct or indirect, in any matter that raises or may raise a conflict with my duties as a manager of my office Management
Conflicts of Interest
The authors declare that they have no conflict of interest.
Financial support and sponsorship
No Funding was received to assist with the preparation of this manuscript
References
- One Global fitness employer 2008-2013 Action Plan for the global method for the Prevention and Manipulation of non-communicable diseases. International Health Corporation, 2008.
View at Publisher | View at Google Scholar - Hu DY, Pan CY, Yu JM The connection between coronary artery disease and peculiar glucose regulation in China: the Chinese coronary heart survey. Eur coronary heart J 2006; 19: 19.
View at Publisher | View at Google Scholar - Bartnik M, Ryden L, Ferrari R, Malmberg good enough, Pyorala ok, Simoons M, et al. The prevalence of normal glucose regulation in patients with coronary artery sickness throughout Europe: the Euro Coronary Heart Survey on Diabetes and the Heart. Eur coronary heart J 2004; 25: 1880 – 1990.
View at Publisher | View at Google Scholar - Global Diabetes Federation. Diabetes Statistics and Figures http://www.diabetes atlas.org/content material/diabetes - and - impaired - glucose - tolerance. Accessed eight January 2010.
View at Publisher | View at Google Scholar - International Diabetes Federations (IDF). Diabetes Atlas. http:// www.eatlas.idf.org/atlas.html?identification=0; 2007.
View at Publisher | View at Google Scholar - Jonsson B., Revealing the Rate of Kind II Diabetes in Europe. Diabetologia 2002 ; 45 : S5–12.
View at Publisher | View at Google Scholar - American Diabetes Association (ADA). National Diabetes Truth Sheet.http://www.cdc.gov/diabetes/pubs/pdf/ndfs_2005.pdf ed; 2005.
View at Publisher | View at Google Scholar - 8He J, Gu D, Wu X, et al. Primary causes of loss of life among women and men in China. N Engl J Med 2005 ; 353: 1124–1134.
View at Publisher | View at Google Scholar - Imposes DCCT lessons. document of a countrywide workshop under the auspices of the British Diabetic Association. Diabet Med1994; 11: 220–228.
View at Publisher | View at Google Scholar - UK Prospective Diabetes Study (UKPDS) group. Intensive blood glucose control with sulfonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998; 352: 837 – 853.
View at Publisher | View at Google Scholar - United Kingdom Prospective Diabetes Examine (UKPDS) organizations. Efficacy of atenolol and captopril in reducing the risk of macro vascular and microvascular complications in type 2 diabetes: UKPDS 39. Br Med J 1998 ;317: 713 – 720.
View at Publisher | View at Google Scholar - Global Diabetes Federation (IDF). The global guiding principle for type 2 diabetes. 2005 [updated 2005; cited 2009]; Available from: http://www.idf.org/Global_guideline .
View at Publisher | View at Google Scholar - Gaede P, Vedel P, Parving HH, Pedersen O . Intensified multifactorial intervention in patients with type 2 diabetes mellitus and Microalbuminuria: the Steno type 2 randomized observation Lancet 1999;353: 617 – 622.
View at Publisher | View at Google Scholar - Saaddine JB, Engelgau MM, Beckles GL, Gregg EW, Thompson TJ, Narayan KM. A Diabetes Document Card for America: Quality of Care in the Nineties. Ann Intern Med 2002; 136: 565 – 574.
View at Publisher | View at Google Scholar - Diabetes manipulation and headaches Trial/Epidemiology of Diabetes Interventions and study institutions. Retinopathy and nephropathy in patients with type 1 diabetes four years after the intensive therapy trial N Engl J Med 2000; 342: 381 – 389.
View at Publisher | View at Google Scholar - Nathan D, Cleary P, Backlund J, et al. Extensive diabetes remedies and cardiovascular ailments in patients with type 1 diabetes. N Engl J Med 2005 ; 353 : 2643 – 2653 .
View at Publisher | View at Google Scholar - Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA . 10 - year follow - up of extensive glucose manipulation in type 2 diabetes. N Engl JMed 2008; 359: 1577 – 1589.
View at Publisher | View at Google Scholar - Gaede P, Vedel P, Larsen N, Jensen GV, Parving HH, Pedersen O . Multifactorial intervention and cardiovascular disorders in patients with type 2 diabetes. N Engl J Med 2003 ; 348 : 383 – 393 .
View at Publisher | View at Google Scholar - Gaede P, Lund - Andersen H, Parving HH, Pedersen O . Impact of multifactorial intervention on mortality in type 2 diabetes. N Engl J Med 2008; 358: 580 – 591.
View at Publisher | View at Google Scholar - Saaddine JB, Cadwell B, Gregg EW, Engelgau MM, Vinicor F, Imperatore G, et al. Upgrades in diabetes approaches of care and intermediate results: United States. 1988 – 2002. Ann Intern Med2006; one hundred forty-four:465 – 474.
View at Publisher | View at Google Scholar - Dodd A, Colby M, Boye okay, Fahlman C, Kim S, Briefel R . Treatment approach and HbA1c manipulation among US adults with type 2 diabetes: NHANES 1999 – 2004. Curr Med Res Opin 2009; 25: 1605 – 1613.
View at Publisher | View at Google Scholar - Persell SD, Zaslavsky AM, Weissman JS, Ayanian JZ. Age-related differences in preventive care among adults with diabetes. Am J Med 2004; 116: 630 – 634.
View at Publisher | View at Google Scholar - Wexler DJ, Grant RW, Meigs JB, Nathan DM, Cagliero E . Sex disparities in the treatment of cardiac chance factors in patients with type 2 diabetes. Diabetes Care 2005; 28: 514 – 520.
View at Publisher | View at Google Scholar - Chan JC, Gagliardino JJ, Baik SH. Multifaceted determinants for accomplishing glycemic control: International Diabetes management exercise observed (IDMPS). Diabetes Care 2009; 32: 227 – 233.
View at Publisher | View at Google Scholar - Harris MI, Eastman RC, Cowie CC, Flegal KM, Eberhardt MS . Racial and ethnic differences in the glycemic management of adults with type 2 diabetes. Diabetes Care 1999; 22: 403 – 408.
View at Publisher | View at Google Scholar - Eeg - Olofsson K, Cederholm J, Nilsson P, Gudbjornsdottir S, Eliasson B . Glycemic and danger factor control in type 1 diabetes: effects from 13,612 patients with a countrywide diabetes sign-up. Diabetes Care 2007;30: 496 – 502.
View at Publisher | View at Google Scholar - Valk GD , Renders CM , Kriegsman DM , Newton KM , Twisk JW , van Eijk JT, et al. Satisfactory taking care of patients with type 2 diabetes mellitus within the Netherlands and the USA: An assessment of two pleasant development applications. fitness Serv Res 2004; 39: 709 – 725.
View at Publisher | View at Google Scholar - Chin MH, Auerbach SB, cook S, Harrison JF, Koppert J, Jin L, et al. High-quality diabetes care in network fitness facilities. Am J Public Fitness 2000; 90: 431 – 434.
View at Publisher | View at Google Scholar - Acton KJ, Shields R, Rith - Najarian S, Tolbert B, Kelly J, Moore K, et al. Making use of the diabetes satisfactory development challenge indicators in the Indian fitness provider number one care putting. Diabetes Care 2001; 24: 22 – 26.
View at Publisher | View at Google Scholar - Sawin CT, Walder DJ, Bross DS, Pogach LM. Diabetes manners and final result measures within the Department of Veterans Affairs. Diabetes Care 2004; 27 ( Suppl 2 ): B90 – 94.
View at Publisher | View at Google Scholar - Eliasson B, Cederholm J, et al.. The distance among recommendations and reality: kind 2 diabetes in a national Diabetes sign-up, 1996 – 2003. Diabet Med 2005 ; 22 : 1420 – 1426 .
View at Publisher | View at Google Scholar - Khunti ok, Ganguli S, Baker R, Lowy A . Capabilities of primary care related to versions in method and final results of care of human beings with diabetes. Br J Gen Pract 2001; 51: 356 – 360.
View at Publisher | View at Google Scholar - Kong AP, Yang X, Ko GT, So WY, Chan WB, Ma RC, et al. Consequences of treatment targets on the next cardiovascular occasions in Chinese patients with type 2 diabetes. Diabetes Care 2007; 30: 953 – 959.
View at Publisher | View at Google Scholar - Chuang LM, Tsai ST, Huang T, and Tai TY The fame of diabetes control in Asia: a flow-sectional survey of 24 317 sufferers with diabetes mellitus in 1998. Diabet Med 2002; 19: 978–985.
View at Publisher | View at Google Scholar - Pan C, Yang W, Jia W, Weng J, and Tian H. Management of Chinese language patients with type 2 diabetes, 1998–2006: the Diabcare–China surveys. Curr Med Res Opin 2009; 25: 39–45.
View at Publisher | View at Google Scholar - Craig M, Jones T, Silink M, and Ping Y Diabetes care, glycemic manipulation, and complications in children with type 1 diabetes from Asia and the Western Pacific region. J Diabetes Complications 2007; 21: 280–287.
View at Publisher | View at Google Scholar - Harris MI. fitness care and health fame and outcomes for sufferers with type 2 diabetes. Diabetes Care 2000; 23: 754–758.
View at Publisher | View at Google Scholar - Lohr KN, Schroeder SA A method for pleasant assurance in Medicare. N Engl J Med 1990; 322: 707–712.
View at Publisher | View at Google Scholar - Lohr KN, Harris-WWehling J. Medicare: a method for quality assurance I. A recapitulation of the has a look at and a definition of quality care. QRB Qual Rev Bull 1991; 17: 6–9.
View at Publisher | View at Google Scholar - Tuttleman M, Lipsett L, and Harris MI Attitudes and behaviors of number one care physician regarding tight manipulation of blood glucose in IDDM sufferers. Diabetes Care 1993; 16: 765–772.
View at Publisher | View at Google Scholar - Weiner JP, Parente ST, Garnick DW, Fowles J, Lawthers AG, Palmer RH version in office: primarily based completely on a claims-based philosophy of care supplied to Medicare patients with diabetes. JAMA 1995; 273:1503–1508.
View at Publisher | View at Google Scholar - Tabak AG, Kerenyi Z, Penzes J, and Tamas G. Awful degree of care among Diabetic sufferers: is that a very precise photograph? Diabetes Care 1999; 22: 533–535.
View at Publisher | View at Google Scholar - Beccles GL, Engelgao MM, Venkat Narayan KM, Hermann WH, Oberth RE, and Williamson DF. A population-based survey of diabetes treatment levels among adults in the United States. Diabetes Care 1998; 21:1432–1438
View at Publisher | View at Google Scholar - Rosenblatt RA , Baldwin LM , Chan L , Fordyce MA , Hirsch IB , Palmer JP, et al Improving the quality of outpatient care in elderly patients with diabetes: Lessons learned from the comparison of rural and urban communities.Journal of Family Medicine 2001; 50:676–680.
View at Publisher | View at Google Scholar - Process Evaluation and Research as a future tool to improve diabetes care. Diabetes Research Clinic Practice 2002; 56:207–211. Item
View at Publisher | View at Google Scholar - Simon LP, Albright A, Behrman MJ, Tom E, Rideout JA.Article Penalties Article Diabetes Treatment Penalties 1999; 22: 208–212.
View at Publisher | View at Google Scholar - [Outpatient care of diabetic patients in 2001. Analysis of the health insurance model of Hessen AOK / Hessen KV individuals Dtsch Med Wochenschr 2003; 128: 2638–2643
View at Publisher | View at Google Scholar - Wetzler HP, Snyder JW. Section links pharmacy and clinical records for evaluation of adequate care for patients with diabetes. DiabetesNursing2000;23:16371641 .
View at Publisher | View at Google Scholar - Simon LPS, Albright A, Behrman MJ, Tom E, Rideout JA.Article Penalties Article Diabetes Treatment Penalties 1999; 22: 208–221.
View at Publisher | View at Google Scholar - Diabetes in Hospitals Diabetes Is There Better Treatment Than General Hospital? Diabetes Care 1997; 20:472-475
View at Publisher | View at Google Scholar - Mifi Eld J.A., Reet-Najarian S.J., Acton K.J., Schraer OK.D., Stan R.M., Johnson M.H.'s evaluation of diabetes treatment is consistent with the medical report observed. Diabetes Treatment 1994; 17:918–923.
View at Publisher | View at Google Scholar - Pommer V., Bressel F., Chen F., and Molzan M. Improving end-of-life care for humans with terminal diabetes Renal failure: epidemiological records from Germany Nephrol Dial Transplant 1997; 12:1318–1320.
View at Publisher | View at Google Scholar - El-Kebbi IM, Ziemer DC, Musey VC, Gallina DL, Bernard AM, Philips LS. Diabetes in urban African people. IX. manufacturer compliance with administrative protocols. Diabetes Remedy 1997; 20: 698-703.
View at Publisher | View at Google Scholar - Anonymous. Evaluation: Treatment adherence may additionally reduce mortality.and morbidity. ACP J. club 1998; 128:53.
View at Publisher | View at Google Scholar - Liniger C., Albeanu A., Bloise D., and Assal J.P. once more about the tuning forkDiabetes Med 1990; 7:859–864.
View at Publisher | View at Google Scholar - Sackett D.L., Snow J.O. The price of Compliance and Non-Compliance settlement. In: R. B. Haynes, D. W. Taylor, and D. L. Sackett, eds., settlement in health care. Baltimore: Johns Hopkins University Press, 1979: 11-22.
View at Publisher | View at Google Scholar - Kravitz R.L., Hayes R.D., Sherbourne okay.D., DiMatteo M.R., Rogers W.H., feedback and adherence to the tips of Ordway L. et al.among chronically ill patients. arch intern med 1993; 153: 1869–1878
View at Publisher | View at Google Scholar - Hoskins P.L., Alford J.B., Handelsman D.J., Yue D.C., and Tortoise J.R. The contrast of various diabetes control fashions for regulatory compliance Self-monitoring of blood glucose levels using a glucose meter with reminiscence diabetes Departed in 1988; 11:719 724.
View at Publisher | View at Google Scholar - Cherkoney K.A., Hart L.K. Linking Beliefs to Health models and adherence in diabetic patients. diabetes, I left in 1980. 3:594-598.
View at Publisher | View at Google Scholar - Watkins D.D., Williams T.F., Martin D.A., Hogan M.D., and Anderson E.A. Diabetes test at home. Am J Department of Public Health Health 1967; 57:452-459.
View at Publisher | View at Google Scholar - Glasgow R.E., Anderson R.M. In the treatment of diabetes, one change from regimen to regimen is not enough. You need something completely different. needed. Diabetes Treatment 1999; 22:2090–2092.
View at Publisher | View at Google Scholar - Fisher E, Brownson C, O'Toole M, Shetty G, Anwuri W, Glasgow R. An ecological approach to self-management: a case of diabetes. this is true J. Public Health, 2005; 95: 1523–1535.
View at Publisher | View at Google Scholar - Phillips LS, Branch W.T., Cook SB, Doyle D.P., El-Kebbi IM, Galina D.L., Except. clinical inertia. Ann Intern Med 2001; 135: 825-834.
View at Publisher | View at Google Scholar - Rodondi N., Peng T., Carter A.J., Bauer D.S., Wittinghoff E., Tan S., different. Treatment modification of poorly controlled arterial hypertension, dyslipidemia, and diabetes mellitus. Ann Intern Med 2006; 144:475-484.
View at Publisher | View at Google Scholar - Brown J. B., Nichols G. A., Perry A. Burden of treatment failure Diabetes type 2. Diabetes Treatment 2004; 27:1535–1540.
View at Publisher | View at Google Scholar - Larme A.S., Pew J.A. Attitudes of primary care workers Diabetes mellitus: barriers to implementation of recommendations. Diabetes Treatment 1998; 21:1391-1396.
View at Publisher | View at Google Scholar - Bernard A.M., Anderson L., Cooke S.B., Phillips L. What's inside Should Residents Improve Diabetes Management? diabetes I left in 1999. 22:661-666.
View at Publisher | View at Google Scholar - YajangJCN. Diabetes Co-Treatment: Why Is It Important? opened in Hong Kong in 1997; 19:315-322
View at Publisher | View at Google Scholar - Yajang JCN. Co-Management of Diabetes: What Permit? opened in Hong Kong in 1997; 17:323-330.
View at Publisher | View at Google Scholar - Wagner E.H., Austin B.T., von Korf M. Organization of patient care I have a chronic illness. Milbank Q 1996; 74:511-544.
View at Publisher | View at Google Scholar - Chang J., So V., Yeng S., Ko G., Lau Y., Tsang M. et al. Structured and traditional treatment for the renal endpoint of type 2 diabetes mellitus. The SURE study: A randomized multicenter translational study. Diabetes Treatment 2009; 32:977-982
View at Publisher | View at Google Scholar - Ellrodt G., cook dinner D.J., Lee J., Cho M., Hunt D., Weingarten S. proof-based medicine. Pete 1997; 258:1687 - 1692
View at Publisher | View at Google Scholar - Norris S.L., Nichols P.J., Kaspersen S.J., Glasgow R.E., Engelgau M.M., the effect of ailment and case-control on Jack L. et al. Humans with Diabetes: a systematic assessment. Am J Prev Med 2002;22 (about): 15–38.
View at Publisher | View at Google Scholar - Holman H., Loric okay. sufferers as companions in persistent ailment controlailment: Partnership is a prerequisite for powerful and green fitness care.Care. Br Med J 2000; 320:526-527.
View at Publisher | View at Google Scholar - Johnson S.B. Methodological problems in diabetes research: size settlement. Diabetes treatment 1992; 15: 1658–1667.
View at Publisher | View at Google Scholar - Verlato G., Maggeo M., Bonora E., Corbellini M., Bressan F., De Marco R. Diabetes center attendance is related to a boom over a 5-year duration. Survival prices in diabetic patients. Diabetes remedy 1996;19:211-213.
View at Publisher | View at Google Scholar - Haynes R.B., McKibbon C.A., Kanani R. A scientific assessment of randomized trials of interventions to help patients adhere to prescribed remedies. The Lancet 1996; 348:383-386.
View at Publisher | View at Google Scholar - Weinberger M., Kirkman M.S., Samsa G.P., Shortliff E.A., LandsmanP.B., Cooper P.A. of doors nursing co-intervention primary Care sufferers with NIDDM: consequences on Blood Glucose manipulation and health-associated first-class of existence. J Gen Intern Med 1995; 10:59 -66.
View at Publisher | View at Google Scholar - Bero L.A., Mays N.B., Bargetek okay., Bond ok. expansion of outpatient cares the role of pharmacists and access to health care. Cochrane database1998 device model; 3: CD000336.
View at Publisher | View at Google Scholar - Ober RE, Herman WH, Waters J., Moore W., Sutton D., Peterson clinical control of patients toenhance glycemic control past BL Diabetic patients in medical institutions. Ann Intern Honey 1998; 129:605-612.
View at Publisher | View at Google Scholar - Kinmont A.L., Woodcock A., Griffin S., Shpigal N., Campbell J. Randomized controlled trial of patient-centered treatment for diabetes habitual Care: effect on contemporary fitness and destiny risks: Diabetes treatment in the Diagnostic observation organization. Br Med J 1998;317: 1202-1208.
View at Publisher | View at Google Scholar - So WY, Tong laptop, Ko GT, Leung WY, Chow Chow, Yeung VT, and many others. Protocol-orientated as opposed to modern-day outpatient treatment Survival rates in sufferers with type 2 diabetes. Amj controlled care 2003; 9:606-615.
View at Publisher | View at Google Scholar - Wu JY, Leung WY, Chang S, Lee B, Zee B, Tong Laptop, et al. Efficiency phone consultations with pharmacists to reduce mortality sufferers taking more than one medicines: a randomized managed trial. Br Med J 2006; 333:522.
View at Publisher | View at Google Scholar - Leung Woo. Ya., So V. Ya., Tong P.ok., Chang N.N., Chang D.ok. effects of systematic treatment of pharmacists and diabetes teams on diabetic sufferers Diabetic nephropathy type 2. Am J Med 2005; 118:1414.
View at Publisher | View at Google Scholar - Wagner E. H., Groves T. . Persistent sickness control. Br Med J 2002; 325:913-914.
View at Publisher | View at Google Scholar - Weingarten S.R., Henning J.M., Badamgarav E., Knight ok., Hasselblad V., Kano A. Jr. et al. Interventions used to treat the ailment applications for human beings with persistent illness - Which programs paintings? Meta-evaluation of published reviews. Br Med J 2002; 325:925.
View at Publisher | View at Google Scholar - Bodenheimer T, Wagner E, Grumbach okay. improving primary care For chronically ill sufferers. Pit 2002; 288: 1775–1779.
View at Publisher | View at Google Scholar - Eckel RH , Grundy SM , Zimmet PZ . The metabolic syndrome. Lancet 2005; 365: 1415 – 1428.
View at Publisher | View at Google Scholar - Adler AI. UKPDS - modeling of cardiovascular risk evaluation and lifetime simulation of outcomes. Diabet Med 2008 ; 25 ( Suppl 2 ): 41 – 46.
View at Publisher | View at Google Scholar - Framingham coronary heart examination. A project of the countrywide coronary heart, Lung and Blood Institute, and Boston College. 1948. to be had from http:// www.framinghamheartstudy.org/.
View at Publisher | View at Google Scholar - Simmons R, Coleman R, rate H, Holman R, Khaw good enough, Wareham N, et al. Performance of the United Kingdom's Ability Diabetes Observes Hazard engine and the Framingham hazard Equations in estimating cardiovascular disease inside the EPIC: Norfolk Cohort. Diabetes Care 2009; 32: 708 – 713.
View at Publisher | View at Google Scholar - Yang XL, So WY, Kong AP, Clarke P, Ho CS, Lam CW, et al. Forestall - level renal sickness danger equations for Hong Kong Chinese language sufferers with kind 2 diabetes: Hong Kong Diabetes Registry. Diabetologia 2006; forty-nine: 2299 – 2308.
View at Publisher | View at Google Scholar - Yang X, Ma RC, So WY, Kong AP, Ko GT, Ho CS, et al. Improvement and validation of a hazard score for hospitalization for coronary heart failure in patients with kind 2 diabetes mellitus. Cardiovasc Diabetol 2008 ;7: 9.
View at Publisher | View at Google Scholar - Yang X, So WY, Tong computer, Ma RC, Kong AP, Lam CW, et al. Development and validation of an all-purpose mortality risk score in kind 2 diabetes. Arch Intern Med 2008; 168: 451 – 457.
View at Publisher | View at Google Scholar - Yang X, So WY, Kong AP, Ma RC, Ko GT, Ho CS, et al. Development and validation of a complete coronary heart illness chance rating in type 2 diabetes mellitus. Am J Cardiol 2008 ; 101 : 596 – 601 .
View at Publisher | View at Google Scholar - Shojania KG, Ranji SR, McDonald KM, Grimshaw JM, Sundaram V, Rushakoff RJ, et al. Consequences of satisfactory improvement Strategies for kind 2 diabetes on glycemic control: a meta-regression analysis. JAMA 2006 ; 296 : 427 – 440 .
View at Publisher | View at Google Scholar - Cagliero E, Levina EV, Nathan DM . On-the-spot comments of HbA1c ranges improve glycemic control in kind 1 and insulin - dealt with the type 2 diabetic patients. Diabetes Care 1999; 22: 1785 – 1789.
View at Publisher | View at Google Scholar - Investigators HOPES. results of ramipril on cardiovascular and microvascular outcomes in human beings with diabetes mellitus: outcomes of the hope observe and MICRO - desire sub-study. Lancet 2000;355: 253 – 259.
View at Publisher | View at Google Scholar - Bakris GL , Weir MR . Angiotensin-converting enzyme inhibitor-associated elevations in serum creatinine: is this a reason for the situation? Arch Intern Med 2000; 160: 685 – 693.
View at Publisher | View at Google Scholar - Palmer BF. coping with hyperkalemia caused by inhibitors of the renin-angiotensin-aldosterone system. N Engl J Med 2004 ; 351 :585 – 592 .
View at Publisher | View at Google Scholar - Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-year compliance with - up of intensive glucose manipulates in type 2 diabetes. N Engl J Med 2008; 359: 1577 – 1589.
View at Publisher | View at Google Scholar - Grey AM, Clarke P. The financial analyses of the UK potential diabetes examination. Diabet Med 2008; 25 ( Suppl 2 ): 47 – 51.
View at Publisher | View at Google Scholar - CDC Diabetes cost-effectiveness group. fee - effectiveness of extensive glycemic manipulation, intensified high blood pressure management, and serum LDL cholesterol level discount for type 2 diabetes. JAMA 2002 ;287: 2542 – 2551.
View at Publisher | View at Google Scholar - Chin MH, Zhang JX, Merrell okay. Diabetes in the African - American Medicare populace: morbidity, first-rate care, and aid utilization. Diabetes Care 1998; 21: 1090 – 1095.
View at Publisher | View at Google Scholar - American Diabetes affiliation. standards of medical care in diabetes, 2009. Diabetes Care 2009; 32 ( Suppl 1 ): 13 – 61.
View at Publisher | View at Google Scholar - Canadian Diabetes Association. medical exercise tips, 2008. to be had from: http://www.diabetes.ca/for-experts/ resources/2008-CPG/.
View at Publisher | View at Google Scholar - country-wide Institute for Health and Clinical Excellence (excellent). kind 2 Diabetes: a countrywide scientific guideline for management in primary and secondary care (replace). 2008. to be had from http://guidance.excellent.org.uk/CG66/steerage/pdf/English.
View at Publisher | View at Google Scholar - Rodbard HW, Blonde L, Braithwaite SS, Brett EM, Cobin RH, Handelsman Y , et al. American affiliation with scientific endocrinologists' medical guidelines for medical exercise for the control of diabetes mellitus. Endocr Pract 2007; 13 ( Suppl 1 ): 1 – 68.
View at Publisher | View at Google Scholar - Jennings ok , Miller KH , Materna SB . changing fitness Care: the growing day after today’s winning fitness firms nowadays. Santa Monica, CA: information change, 1999.
View at Publisher | View at Google Scholar
