

Research Article | DOI: https://doi.org/10.31579/2835-7957/006
Stress and Anxiety Among Caregivers of Home-Isolated and Hospitalized COVID-19 Patients: A cross-sectional study from 11 countries worldwide
- Nancy Ruíz-Domínguez 1*
- Mahmoud Bassiony 2
- Yana Al-Inaya 3
- Chrysi Mandola 4
- Juan Carlos Ayala-Alvarez 5
- Maya Abdelwahab 6
- Rehab E. Ashmawy 7
- Meena Faiez Assad 8
- Michael Azeze Negussie 9
- Aya Mustafa Dawood 10
- Koppineedi Satya Bharathi 9
- Alaa Akrm Ahmed Hassanin El Marakby 6
1 Faculty of Medicine, Alexandria University, Egypt.
2 Department of Medicine and Nutrition, University of Guanajuato, León, Guanajuato, Mexico.
3 Grigore T. Popa, University of Medicine and Farmacy, Iasi, Romania.
4 Faculty of Medicine, Uzhhorod National University, Ukraine
5 Universidad de Guadalajara, Guadalajara, Jalisco, México
6 Faculty of Medicine, Helwan University, Cairo, Egypt
7 Faculty of Medicine, Ain-Shams University, Cairo, Egypt
8 School of Medicine, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia
9 Government Medical College Surat, India
10 Faculty of Dentistry, October 6 University, Cairo, Egypt
*Corresponding Author: Nancy Ruíz-Domínguez, Faculty of Medicine, Alexandria University, Egypt.
Citation: Nancy Ruíz-Domínguez, Mahmoud Bassiony, Yana Al-Inaya, Chrysi Mandola, Juan Carlos Ayala-Alvarez. (2022). Stress and Anxiety Among Caregivers of Home-Isolated and Hospitalized COVID-19 Patients: A cross-sectional study from 11 countries worldwide. Clinical Reviews and Case Reports.1(2); DOI:10.31579/2835-7957/006
Copyright: © 2022 Nancy Ruíz-Domínguez, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27 October 2022 | Accepted: 04 November 2022 | Published: 29 November 2022
Keywords: anxiety; caregivers; multination, pandemic; stress
Abstract
Background: With the focus on vaccines, novel treatments, and prevention of infection during COVID-19 pandemic, there has been less identification of mental health disorders. The uncertainty of when this pandemic will be over only increases stress, anxiety and other mental disorders worldwide, not only on patients, but also within their household members. Thus, we aim to further investigate the prevalence of stress and anxiety among COVID-19 patients’ family members.
Methods: A multinational cross-sectional study to evaluate stress and anxiety among COVID-19 patients' non-health care professionals’ caregivers among 11 different countries. The self-reported PSS-10 and GAD-7 have been used as outcome measures.
Results: Collected data revealed that the mean values for PSS (p less than0.001) and GAD-7 (p less than0.001) scores were higher in families of hospitalized patients. Higher average scores observed in male population for GAD-7, female population for PSS, and lower-income groups, suburban regions, and prolonged duration of infection for both scales. The United States displayed the highest scores, while Indonesia and Poland reported the lowest scores on GAD-7 and PSS respectively. Main concerns expressed by family members were the spread of infection in the family (57.74Percentage), potential death (51.18Percentage), and health services’ availability (46.3Percentage). Discussion with closed ones (36.17Percentage) and physical exercise (24.93Percentage) mentioned as main coping strategies.
Conclusion: Anxiety and stress represent a major consequence of the COVID-19 pandemic, burdening family members to a great extent. Thus, immediate attention to this matter is in order with appropriate action to ensure the mental health of these caregivers.
Introduction
With over 258 million cases of COVID-19 documented all around the world, a state of pandemic has been declared by the WHO in March 2020. Consequently, COVID-19 has put many countries in a state of emergency. Numerous studies have been published discussing the physical symptoms and signs seen in the patients since then (del Rio et al., 2020). However, only a few described the psychological and social impacts the virus has had on the patients along with the accompanying symptoms, compared to similar epidemics. (Deng et al., 2021).
These studies have shown that psychological stress is often linked to significant decrease in quality of life. In the past decades, associations and pathways linking psychological distress to disease and pandemics have been studied and well established. Unhealthy lifestyle changes and heightened levels of stress, anxiety, and depression due to pandemic-induced psychological distress may in turn pose significant negative impact on individuals’ mental health (Altena et al., 2020).
COVID-19 has created an environment with profound psychosocial disturbances which develops rapidly among individuals and ranges from mild manifestations of stress, and anxiety with irregular sleep patterns to panic attacks, desperation, negativism, and severe insomnia (Serafini et al., 2020). A recent meta-analysis documented high levels of psychological stress among the general population, whereby approximately one in four adults were found to require mental health services (Cooke et al., 2020). These findings were also echoed in a study conducted during the early phase of COVID-19 pandemic in the Philippines, where one-seventh of the respondents reported moderate-to-severe stress levels (Tee ML et al., 2020). Another study conducted in Austria also revealed that 37.7Percentage of the study population faced severe psychological impact due to COVID-19 (Traunmüller et al., 2020). Several factors are likely to induce anxiety among residents and people affected by COVID-19 themselves or in relation to, including the continual number of confirmed cases and deaths, insufficient knowledge regarding the disease, being surrounded by infected individuals, and the lack of anti-coronavirus specific drugs, among other reasons (Zhang et al., 2020). A study in Hong Kong at the peak of the pandemic outrage between April and May 2020 showed that 19Percentage of the sample population had depression and 14Percentage had anxiety (GAD score ≥10) (Choi et al., 2020).
Nevertheless, COVID-19 has also been a burden for the patients’ close environment in addition to the patients themselves. Family members of COVID-19 patients may have a wide range of physical and mental exhaustion. This is mainly determined by the degree of relationship they have and whether they are directly involved in taking care of the patient during infection. There has been a remarkable increase in the prevalence of stress, anxiety, depression and sleep disorders (condition-specific ranges from 12Percentage to 67.5Percentage) among caregivers and parents (Vizheh et al., 2020). Duration of hospitalization with the subsequent separation from family, severity of the illness and the capacity of health care facilities could be additional risk factors that potentially have significant impact on the caregivers.
Psychological health has been getting attention recently, starting from health care professionals to the public in different sectors. With the noticed increase in patients with mental disorders, increasing public awareness has become a vital priority for health care providers all around the world. Informal caregivers during the pandemic have experienced new, but varying levels of stress, especially with the need for routine change and adapting to home healthcare. There are not sufficient studies that provide information concerning the prevalence of stress and anxiety symptoms in the caregivers of COVID-19 patients. Therefore, This study aims to observe the changes in psychological health during the pandemic, such as stress and anxiety, worldwide (Sheth et al., 2021), accentuating their significant effect on the COVID-19 patients' informal caregivers.
Methodology
Study Design - Cross-sectional study
Sampling - Convenience sampling
Sample size - The sample size of 1250 (625 from each country) was calculated using the Slovin’s formula n = N/ (1 + Ne²), where, n = sample size for each country, N = COVID-19 cases for USA and India as on 15 July 2021 (USA -33 604 822 and India -31 025 878), e = tolerance error ****
Study subjects
Participation was anonymous and voluntary in this study.
Inclusion criteria - covered family members or informal caregivers (Mother, Father, Son, Daughter, Sister, Brother, Grandfather, Grandmother, Granddaughter, Grandson, Mother-in-Law, Father-in-Law, Son-in-Law, Daughter-in-Law, Uncle, Aunt, Niece, Nephew, Wife, Husband, Fiance/Fiancee, Boyfriend, Girlfriend, Significant other, Friend, Neighbour, Teacher, Student, Co-worker, Classmate, Cousin, Other) who were directly or indirectly taking care of the patient.
***Exclusion criteria - people with history of any chronic mental disorder and health care professionals.
Data Collection
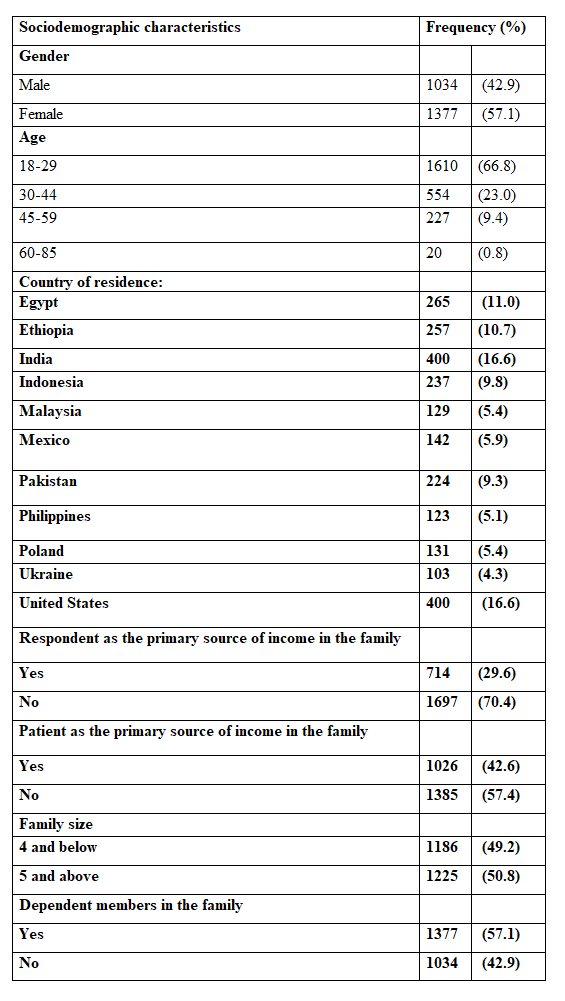
The total number of participants was 2411 from the countries listed in Table 1. Information about the study and its purpose were described and informed consent was taken from each participant. Participants filled out an online questionnaire via Google Form composed of 12 sections assessing mental health. In addition, the survey collected demographic data which includes age, gender, marital status, occupation of caregiver and patient, country, state, city, area of residence, education level and income group, as well as information regarding major factors affecting the mental health of the caregivers and common concerns shared by families of COVID-19 patients. In order to ensure uniformity and validity of the scales used, the survey was fully developed in English.
Study tools
The psychological responses from the family/primary caregiver were assessed using two established assessment tools:
Perceived Stress Scale (PSS-10): A self-report scale which is utilised to measure perception of stress among respondents during the preceding month. The scale contains 10-items and is scored between 0 to 40, with higher scores pointing towards greater risk for future distress. (Cohen, Kamarck, & Mermelstein, 1983).
General Anxiety Disorder-7 (GAD-7): A 7-item anxiety measure whereby each item is scored between 0 to 3. The whole scale score ranges from 0 to 21, with cut off scores for mild, moderate and severe anxiety at 5, 10, and 15 respectively. The scale has a 89Percentage sensitivity and 82Percentage specificity for Generalised Anxiety Disorder. (MIRECC).
Results
Our study had a total of 2411 participants from across 11 countries among whom 42.9Percentage (1034) were male and 57.1Percentage (1377) were female. Regarding socio-economic status, the majority reside in urban areas (81Percentage) and belong to middle-income groups (77.9Percentage). The most common age groups of our respondents were between 18-29 (66.8Percentage) and 30-44 (23Percentage). Among 42.6Percentage (1026) of the respondents, the primary source of income in the family was the patient. More details about the demographic characteristics of our population are illustrated in table 1. All additional information related to table 1 results can be found in the online resource 1. A significant number in our population (47.7Percentage) stated a negative psychological impact on their mental health during the period of the COVID-19 pandemic.
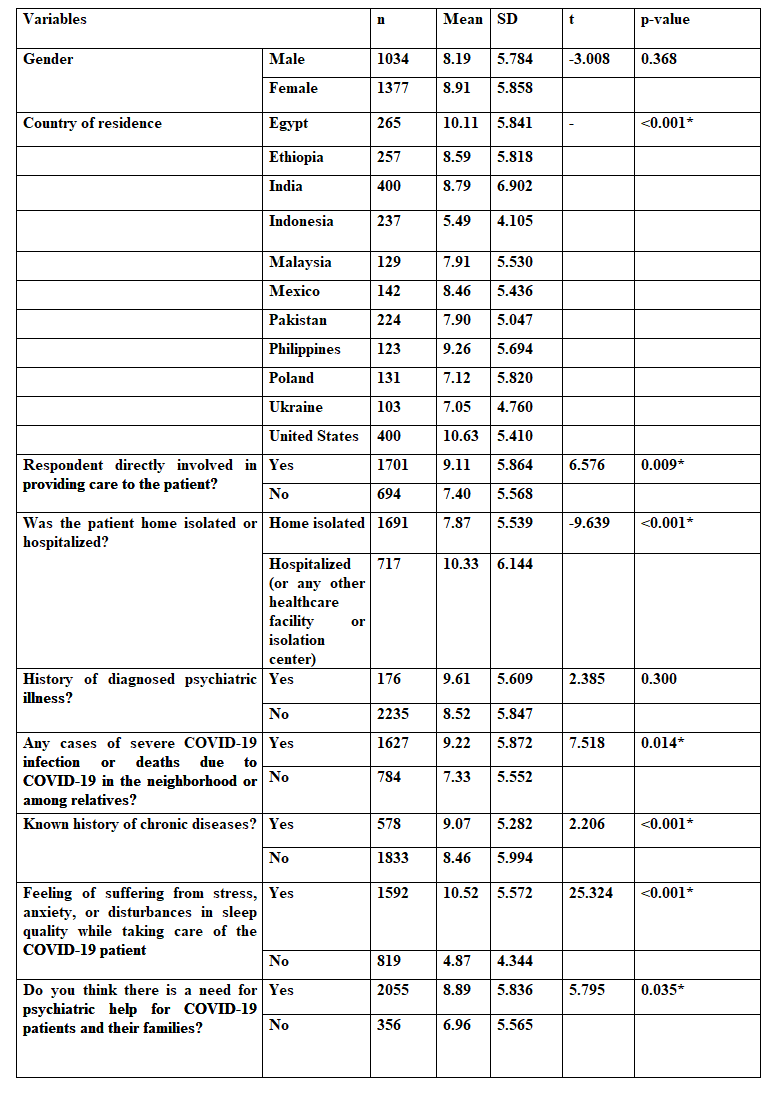
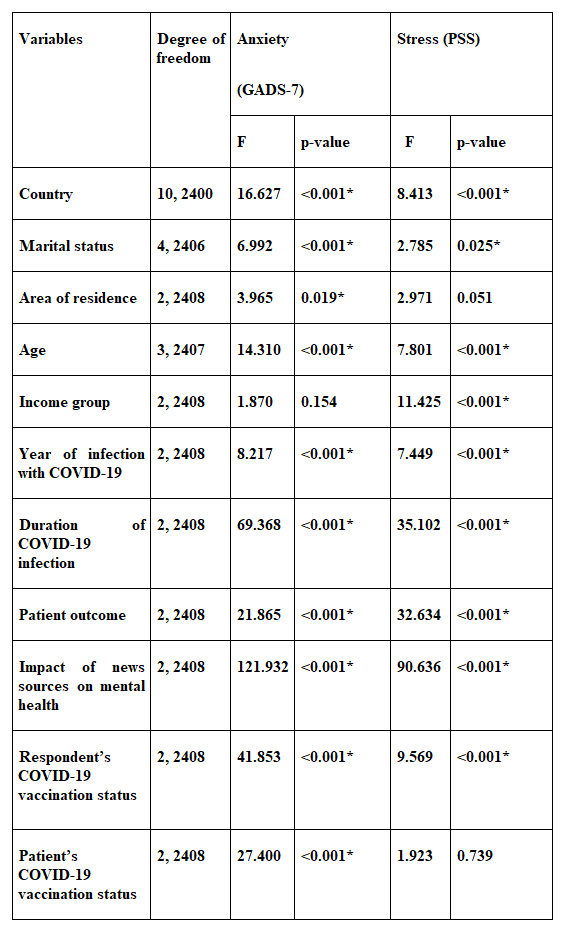
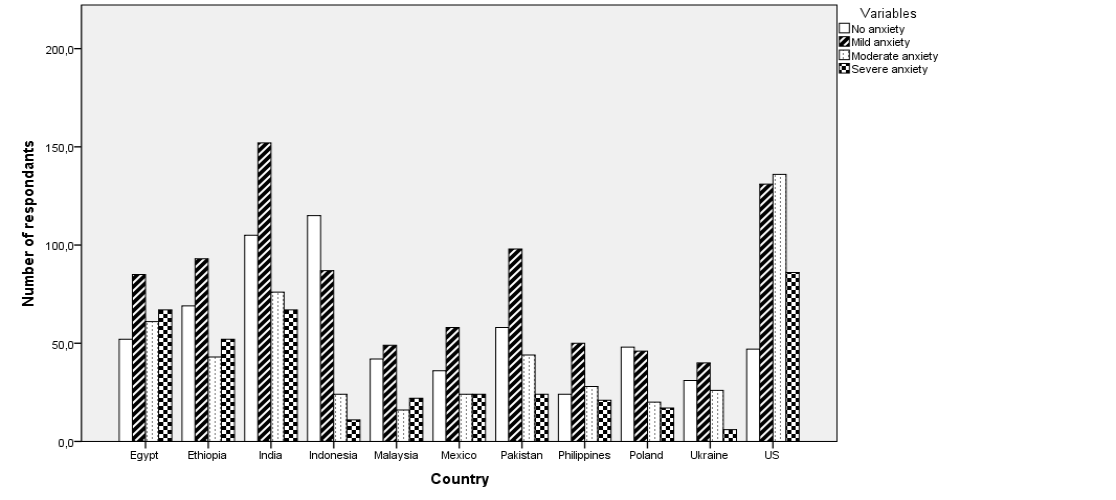
In more detail, evaluation of anxiety was performed through The Generalized Anxiety Disorder-7 Score (GADS-7). According to figure 1, the most common clinical presentation was moderate anxiety, with highest prevalence in the United States (34.0Percentage) among the eleven countries, followed by Egypt (23Percentage) and India (19Percentage). The lowest levels of anxiety were observed in Malaysia (12.4Percentage). In table 2, certain risk factors were proven to have statistical significance for anxiety development. These are direct caregivers (p=0.009), patient’s hospitalization (p less than0.001), previous experience with severe COVID-19 infection or death (p=0.014) and family size of 4 and below (p=0.014). Information regarding table 2 can be found in the online resource 2. Main concerns of patients can where analyzed and described in figure 5 (Online resource 5). Additional significant variables were 30-44 age group (p less than0.001), residence in suburban areas (p=0.019), married as marital status (p less than0.001), 2020 as the year of COVID infection (p less than0.001) and the duration and possible outcome of the infection (p less than0.001), as mentioned, while full vaccination status was seemed to minimize feelings of anxiety in figure 4 which can be found in online resource 6. Symptoms referred by caregivers are added in the online resource 7.
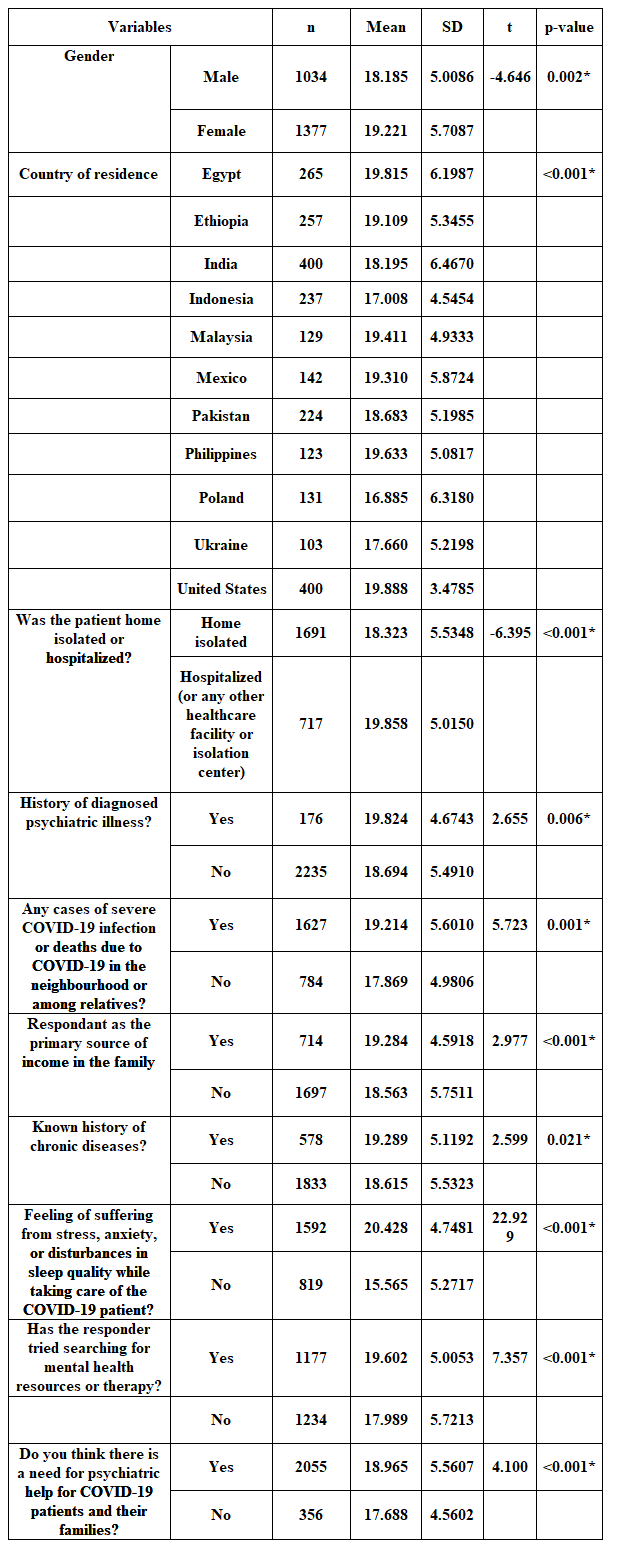
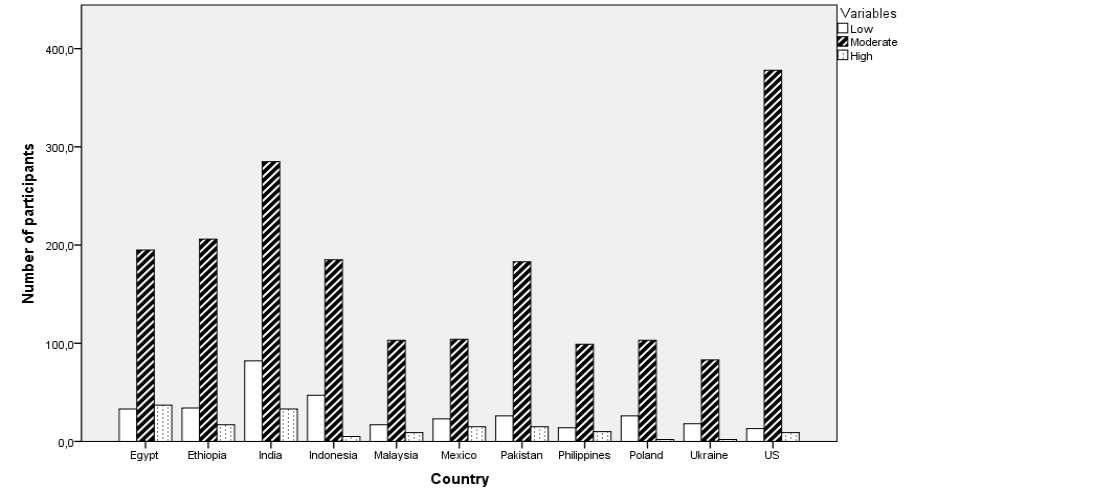
Regarding stress statistics among caregivers, clinical diagnosis of stress was based on the results of PSS-10, with moderate stress as the most frequent. From figure 2, the highest percentage was found in the USA population (94.5Percentage), followed by India (285) and Ethiopia (208), with the lowest rate found in Ukraine (83). As indicated in table 3, stress was precipitated by female sex (p=0.002), patient’s hospitalization (p less than0.001), co-morbidities (p=0.021) and previous experience with severe COVID-19 infection or death (p=0.001). Additional information regarding table 3 can be found in online resource 3. From table 4, statistical significance was observed between stress manifestation and low income (p less than0.001), age 30-44 (p less than0.001), year and duration of COVID-19 infection (p less than0.001) and patient’s outcome (p less than0.001). In addition, full vaccination status is considered a positive influence on caregivers' mental health, as shown on table 4.
All additional information on results analysis can be found in online resources 1-7.
Discussion
In the US, a study with 1978 participants demonstrated anxiety prevalence at 42Percentage (Khubchandani et al., 2021) which is identified in our study with the highest prevalence. In the Indian population, frequent mental disorders documented are related with anxiety and stress.. Similar countries present with high anxiety levels, such as Mexico, documented by one study with 613 subjects (Pérez-Cano et al., 2020) and another with a total of 1667 patients where 632 had anxiety (Hernandez et al., 2021) , and Pakistan with generalized anxiety to be identified in a great percentage among the general population (Riaz, M. et al., 2021) (Anzar et al., 2020). Economic impact of repeated lockdown strategies is a major component in developing mental health issues in India (Rehman et al., 2021), with low-income households being an important risk factor in our study as well. Low-income factor is identified also in Egypt population (Arafa et al., 2021) (Elkayal et al., 2022), the second country with the highest anxiety percentages in our study. Additional significant risk factors identified for anxiety development were a direct caregiver relation, duration of patient hospitalization and a previous experience with SARS-COV2 infection. Anzar et al. shows generalized anxiety disorders are high among the general population, whereas other symptoms like sleep disturbance and depression are low. Regarding stress, prevalence among our countries reported moderate stress as most frequent, being highest in the US population (94.5Percentage), followed by India (Rehman et al., 2021), Ethiopia, which is comparable with two different studies, with more than 30Percentage reported cases of stress disorder (Ayalew et al., 2021)(GebreEyesus et al., 2021), and Philippines with a high percentage of moderate stress, supported by Idris & Akhir 2021 stating that caregivers suffer from psychological distress (Idris & Akhir, 2021). A systematic review and Meta-regression with 29 studies and a sample size of 22,380, reported prevalence of stress in 9 studies among COVID-19 caregivers (Salari et al., 2020), and another study, which is supporting our findings, is a Mexican study with 1667 patients, and reported moderate stress as the most prevalent (Hernandez et al., 2021). We highlighted that females experience higher levels of stress, which can be attributed to two possible explanations (Riaz, M. et al., 2021) (Anzar et al., 2020). First, women represent the primary caregiver in a household, and additional responsibilities and burden due to home isolation policy, can contribute to development of distress feelings (Anand et al., 2021). Another explanation may be the increased incidence of domestic violence in the pandemic period (Gausman & Langer, 2020). A higher incidence of mental health problems studied, was observed in younger age groups. These may occur due to the access to massive amounts of information related to the COVID-19 pandemic (Anand et al., 2021) (Arafa et al., 2021). Continuous exposure to all kinds of knowledge may create a state of fear and uncertainty, predisposing to mental health issues (Elkayal et al., 2022). However, a study in Poland mentioned that older populations are reporting higher stress levels (Sozański et al., 2021), which comes in contrast with our findings. Due to the absence of a proper healthcare system and facilities worldwide, family caregivers were not adequately attended to, leading to an increased prevalence in mental health disorders such as the ones approached in this study. (Bergmann & Wagner, 2021) (Muldrew et al., 2021). A cross-sectional study from Indonesia that compared knowledge, attitudes and practices toward anxiety during the pandemic, with 1082 participants in questionnaires, showed that anxiety was higher in participants who disagreed with Indonesia having control of COVID -19 and those who practiced going to crowded places (Rias et al., 2020). It is reasonable to assume that the confidence in pandemic control would play an important role in participants as a risk factor for presenting general anxiety. Due to fear of contamination, either admissions to the hospital were decreased or patients were discharged more rapidly, creating a new state of home care. As a result, family caregivers were overloaded with great responsibilities and additional pressure. They are required to provide courage and strength to the patient, so an extra effort to hide their own fear and keep an optimistic attitude with subsequent suppression of their own negative feelings, can predispose to mental health problems (Rahimi et al., 2021). In this study, direct caregiving was found to be a significant risk factor for anxiety and stress in Ukraine, Poland (Bergmann & Wagner, 2021), India (Muldrew et al., 2021), Egypt (Arafa et al., 2021) and Indonesia (Rias et al., 2020).
Conclusion
The reported high prevalence of mental health disorders arises as an immense public health issue, which exceeds all expectations and requires immediate attention with preventive and therapeutic strategies to be addressed (Lakhan et al., 2020). The first step in management of psychological health disorders is identifying the problem, in this case, stress and anxiety. Our study shows a direct cause-effect of pandemics, such as COVID-19, on worldwide mental health. The results of this study demonstrate that the prevalence of stress and anxiety in caregivers of patients with COVID-19 is significant and requires correct identification and management so that it does not interfere with the individual's daily life.
In conclusion, our study supports the idea of the significant negative effect of the COVID-19 pandemic on the mental health of family members who were taking care of patients infected with coronavirus worldwide. It revealed a high prevalence of anxiety and stress among family caregivers. These findings suggest that monitoring and preventing mental health disorders is crucial. Several approaches are needed to reduce and treat Family caregivers’ mental health disorders. Further research is required to identify these approaches to prevent and treat these disorders in family members of COVID-19 patients.
Future Prospect
More research should be conducted on how the mental health of caregivers of COVID-19 patients has been impacted by the pandemic. Considering the unexpected length and severity of this pandemic as well as the huge proportion of respondents experiencing anxiety and stress, it is imperative that these concerns are adequately explored and addressed. Future research should also focus on this population, as they are particularly vulnerable and play a crucial role in combating this pandemic. Results of the studies may be utilized to facilitate the commencement of evidence-based intervention to prevent further mental health complications in this population.
Limitations
The generalizability of our findings may be impacted by several limitations. Some of the findings may be biased due to self-selection by the respondents. Another important limitation in our research is the inability to prove a temporal relationship between exposure and outcome, which are assessed simultaneously, owing to its cross-sectional nature. Hence, it may be difficult to form predictive conclusions based on the results. The language utilized in our data collection form (English) may affect the response garnered in a non-English speaking country. The survey was disseminated via online platforms and thus may pose some limitations in terms of outreach. Moreover, convenience sampling was used to collect our study response which may also limit the ability of the study to produce representative results for our target population.
Additional studies must be conducted to identify mental health profiles in the general population, and to provide support and problem-solving aid to individuals presenting anxiety, stress, and sleep disorders. This study provides insight on factors (occupation, economic status, marital status, vaccination status, sex, patient hospitalization, previous experience of infection, etc.) predisposing to the disorders in caregivers during the COVID-19 pandemic, showing the overwhelming prevalence around the world. Despite having 2411 participants, a larger sample and more resources are needed for a precise representation of the world population. A study of 5065 US adults in March 2020 indicated that among the states with more than 50 COVID-19 cases, each additional day of isolation was associated with an 11Percentage increase in the odds of moving up a category of psychological distress [6]. The increase in variants is important for future pandemic phases, there might be moments where isolation may continue and others in which it may not, which could be a determinant for a change in results.
Acknowledgments
We express our thoughtful gratitude to Prof. Dr. Maha Ghanem, Chairman of Ethics Committee at the Alexandria Faculty of Medicine, for her help in the IRB approval process. We are also deeply thankful to Innores International Cohort (Yashendra Sethi, Oroshay Kaiwan, Mahmoud Bassiony, Nafisa Turabi, Vidhi Vora, Pratik Agarwal, Neeraj Gajwani, Ishwarya V, Fernanda Ambriz-Salas, Daniel Ehis Aibonoga, Hussam Kiwan, Hanusha Durganaudu, Onyekachi Emmanuel Anyagwa, Miguel Angel Palacios-Garay, Snehal Gohel, Keshav Garg, Aakansha Singh, Bhawdeep Singla, N Nishitha Ramesh, Freya Kankhara, Sudipta Pal, Hoda Walid ElHammady, Shubham Madan, Shraddha Goyal, Udithi Bandaru, Paraskevi Samouti, Siva Sai Belagallu, Adyut Prakash,
Debabrata Roy, Kartik Gohel, Eman Khaled, Moshi Moshi Shabani, Akshay Jitendrabhai Gajjar, Richa Ashish Ganatra, Amruth Srinivasaagrahara Krishnegowda, Umair Khursheed, Galih Ricci Muhammad, Cristopher Moises Cano-Gonzalez, Giancarlo Bolledi, Mohommad Rayan Rais, Magdalena Kras, Jade Simpson, Habiba Samy Farag, Ambar Suclly Calderon, Ifat Mabruka, Ahmed K. Awad and Taqwa Emad Alden) for their help in distributing the questionnaire and their support during the study. Finally, we highlight the outstanding contribution of our collaborators body (Abed Nego Okthara Sebayang from Indonesia, Faiqa Zaki from Pakistan, Lim Jia Jia from Malaysia, Feven Mekonnen, Fitsum Assefa and Sabrina Zeleke Belay from Ethiopia, Oliwia Dalek from Poland, and Janelle Britanny Go from Philippines) in data collection among their respective countries.
Declarations
Funding
No funding was received for conducting this study.
Competing interests
The authors have no competing interests to declare that are relevant to the content of this article.
Ethics approval
The approval was obtained from the Ethics Committee of the Faculty of Medicine, Alexandria University - IRB NO.: 00012098. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Consent to participate
Consent was obtained from participants included in the study.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Statements and Declaration
The authors did not receive support from any organization for the submitted work. All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
References
- Altena, E., Baglioni, C., Espie, C. A., Ellis, J., Gavriloff, D., et al. (2020). Dealing with sleep problems during home confinement due to the COVID‐19 outbreak: Practical recommendations from a task force of the European CBT‐I Academy. Journal of Sleep Research, 29(4).
View at Publisher | View at Google Scholar - Anand, V., Verma, L., Aggarwal, A., Nanjundappa, P., & Rai, H. (2021). COVID-19 and psychological distress: Lessons for India. PLOS ONE, 16(8), e0255683.
View at Publisher | View at Google Scholar - Arafa, A., Mohamed, A., Saleh, L., & Senosy, S. (2021). Psychological Impacts of the COVID-19 Pandemic on the Public in Egypt. Community Mental Health Journal, 57(1), 64–69.
View at Publisher | View at Google Scholar - Ayalew, M., Deribe, B., Abraham, Y., Reta, Y., Tadesse, F., et al. (2021). Prevalence and determinant factors of mental health problems among healthcare professionals during COVID-19 pandemic in southern Ethiopia: multicentre cross-sectional study. BMJ Open, 11(12), e057708.
View at Publisher | View at Google Scholar - Bergmann, M., & Wagner, M. (2021). The Impact of COVID-19 on Informal Caregiving and Care Receiving Across Europe During the First Phase of the Pandemic. Frontiers in Public Health, 9.
View at Publisher | View at Google Scholar - Buysse, D. J., Reynolds, C. F., Monk, T. H., Berman, S. R., & Kupfer, D. J. (1989). The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Research, 28(2), 193–213.
View at Publisher | View at Google Scholar - Choi, E. P. H., Hui, B. P. H., & Wan, E. Y. F. (2020). Depression and Anxiety in Hong Kong during COVID-19. International Journal of Environmental Research and Public Health, 17(10), 3740.
View at Publisher | View at Google Scholar - Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A Global Measure of Perceived Stress. Journal of Health and Social Behavior, 24(4), 385.
View at Publisher | View at Google Scholar - Cooke, J. E., Eirich, R., Racine, N., & Madigan, S. (2020). Prevalence of posttraumatic and general psychological stress during COVID-19: A rapid review and meta-analysis. Psychiatry Research, 292, 113347.
View at Publisher | View at Google Scholar - del Rio, C., Collins, L. F., & Malani, P. (2020). Long-term Health Consequences of COVID-19. JAMA, 324(17), 1723.
View at Publisher | View at Google Scholar - Deng, J., Zhou, F., Hou, W., Silver, Z., Wong, C. Y., et al. K. (2021). The prevalence of depression, anxiety, and sleep disturbances in COVID‐19 patients: a meta‐analysis. Annals of the New York Academy of Sciences, 1486(1), 90–111.
View at Publisher | View at Google Scholar - Elkayal, M. M., Shahin, M. A. H., & Hussien, R. M. (2022). Psychological distress related to the emerging COVID-19 pandemic and coping strategies among general population in Egypt. Journal of the Egyptian Public Health Association, 97(1), 3.
View at Publisher | View at Google Scholar - Gausman, J., & Langer, A. (2020). Sex and Gender Disparities in the COVID-19 Pandemic. Journal of Women’s Health, 29(4), 465–466.
View at Publisher | View at Google Scholar - GebreEyesus, F. A., Tarekegn, T. T., Amlak, B. T., Shiferaw, B. Z., Emeria, M. S., et al. (2021). Levels and predictors of anxiety, depression, and stress during COVID-19 pandemic among frontline healthcare providers in Gurage zonal public hospitals, Southwest Ethiopia, 2020: A multicenter cross-sectional study. PLOS ONE, 16(11), e0259906.
View at Publisher | View at Google Scholar - Idris, A., & Akhir, N. M. (2021). COVID-19 Pandemic: Are Caregivers of Family Members with Depression at Risk?.
View at Publisher | View at Google Scholar - Jahrami, H., BaHammam, A. S., Bragazzi, N. L., Saif, Z., Faris, M., et al. (2021). Sleep problems during the COVID-19 pandemic by population: a systematic review and meta-analysis. Journal of Clinical Sleep Medicine, 17(2), 299–313.
View at Publisher | View at Google Scholar - Khubchandani, J., Sharma, S., Webb, F. J., Wiblishauser, M. J., & Bowman, S. L. (2021). Post-lockdown depression and anxiety in the USA during the COVID-19 pandemic. Journal of Public Health, 43(2), 246–253.
View at Publisher | View at Google Scholar - Lakhan, R., Agrawal, A., & Sharma, M. (2020). Prevalence of Depression, Anxiety, and Stress during COVID-19 Pandemic. Journal of Neurosciences in Rural Practice, 11(04), 519–525.
View at Publisher | View at Google Scholar - Muldrew, D. H. L., Fee, A., & Coates, V. (2021). Impact of the COVID‐19 pandemic on family carers in the community: A scoping review. Health & Social Care in the Community.
View at Publisher | View at Google Scholar - Pérez-Cano, H. J., Moreno-Murguía, M. B., Morales-López, O., Crow-Buchanan, O., English, J. A., et al. (2020). Anxiety, depression, and stress in response to the coronavirus disease-19 pandemic. Cirugia y Cirujanos, 88(5), 562–568.
View at Publisher | View at Google Scholar - Rahimi, T., Dastyar, N., & Rafati, F. (2021). Experiences of family caregivers of patients with COVID-19. BMC Family Practice, 22(1), 137.
View at Publisher | View at Google Scholar - Rehman, U., Shahnawaz, M. G., Khan, N. H., Kharshiing, K. D., Khursheed, M., et al. (2021). Depression, Anxiety and Stress Among Indians in Times of Covid-19 Lockdown. Community Mental Health Journal, 57(1), 42–48.
View at Publisher | View at Google Scholar - Rias, Y. A., Rosyad, Y. S., Chipojola, R., Wiratama, B. S., Safitri, C. I., et al. (2020). Effects of Spirituality, Knowledge, Attitudes, and Practices toward Anxiety Regarding COVID-19 among the General Population in INDONESIA: A Cross-Sectional Study. Journal of Clinical Medicine, 9(12), 3798.
View at Publisher | View at Google Scholar - Rodríguez-Hernández, C., Medrano-Espinosa, O., & Hernández-Sánchez, A. (2021). Salud mental de los mexicanos durante la pandemia de COVID-19. Gaceta medica de Mexico, 157(3).
View at Publisher | View at Google Scholar - Salari, N., Khazaie, H., Hosseinian-Far, A., Khaledi-Paveh, B., Kazeminia, M., et al. (2020). The prevalence of stress, anxiety and depression within front-line healthcare workers caring for COVID-19 patients: a systematic review and meta-regression. Human Resources for Health, 18(1), 100.
View at Publisher | View at Google Scholar - Serafini, G., Parmigiani, B., Amerio, A., Aguglia, A., Sher, L., et al. (2020). The psychological impact of COVID-19 on the mental health in the general population. QJM: An International Journal of Medicine, 113(8), 531–537.
View at Publisher | View at Google Scholar - Sheth, K., Lorig, K., Stewart, A., Parodi, J. F., & Ritter, P. L. (2021). Effects of COVID-19 on Informal Caregivers and the Development and Validation of a Scale in English and Spanish to Measure the Impact of COVID-19 on Caregivers. Journal of Applied Gerontology, 40(3), 235–243.
View at Publisher | View at Google Scholar - Sozański, B., Ćwirlej-Sozańska, A., Wiśniowska-Szurlej, A., Jurek, K., Górniak, P., et al. (2021). Psychological responses and associated factors during the initial stage of the coronavirus disease (COVID-19) epidemic among the adult population in Poland - a cross-sectional study. BMC Public Health, 21(1), 1929.
View at Publisher | View at Google Scholar - Tee, M. L., Tee, C. A., Anlacan, J. P., Aligam, K. J. G., Reyes, P. W. C., et al. (2020). Psychological impact of COVID-19 pandemic in the Philippines. Journal of Affective Disorders, 277, 379–391.
View at Publisher | View at Google Scholar - Vizheh, M., Qorbani, M., Arzaghi, S. M., Muhidin, S., Javanmard, Z., et al. (2020). The mental health of healthcare workers in the COVID-19 pandemic: A systematic review. Journal of Diabetes & Metabolic Disorders, 19(2), 1967–1978.
View at Publisher | View at Google Scholar - Zhang, Y., Chen, Y., Wang, J., Deng, Y., Peng, D., et al. (2020). Anxiety Status and Influencing Factors of Rural Residents in Hunan During the Coronavirus Disease 2019 Epidemic: A Web-Based Cross-Sectional Survey. Frontiers in Psychiatry, 11.
View at Publisher | View at Google Scholar
