

Case Report | DOI: https://doi.org/10.31579/2835-7957/016
Plongeant Goiter Short Case Series Description
1 Postgraduate endocrinology. Clinic of Endocrinology and Metabolism. School of Medicine. Hospital of Clinics. UdelaR. Uruguay, Montevideo.
2 Adjunct Professor. Clinic of Endocrinology and Metabolism. School of Medicine. Hospital of Clinics. UdelaR. Uruguay, Montevideo.
3 Associate professor. Clinic of Endocrinology and Metabolism. School of Medicine. Hospital of Clinics. UdelaR. Uruguay, Montevideo.
*Corresponding Author: Gabriela Mintegui, Postgraduate endocrinology. Clinic of Endocrinology and Metabolism. School of Medicine. Hospital of Clinics. UdelaR. Uruguay, Montevideo.
Citation: Martinez Z., Agüero P., Mintegui G., (2023), Plongeant Goiter Short Case Series Description, Clinical Reviews and Case Reports, 2(2); DOI:10.31579/2835-7957/016
Copyright: © 2023, G Acun. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 March 2023 | Accepted: 14 March 2023 | Published: 22 March 2023
Keywords: thyroid gland; renal replacement therapy; neck tumor; pulmonary disease; parkinson's
Abstract
Goiter is an abnormal enlargement of the thyroid gland, produced by multiple causes such as iodine deficiency, autoimmune diseases (Hashimoto, Graves), thyroid nodules or thyroid cancer. When the goiter is partially or totally in the mediastinum, it is called Plongeant goiter, presenting its own symptoms (dysphagia, dysphonia, cough).
Diagnosis is clinical, supported by laboratory and imaging tests to determine its etiology, assess involvement of nearby structures, and propose treatment, with surgery being the one of choice.
A short series of cases of Plongeant goiter is presented, one in a patient with multiple comorbidities, another associated with thyroid cancer, another with hyperthyroidism, and another with significant compromise of the tracheal lumen.
The clinical behavior of each one, and its resolution, are analyzed.
Introduction
The term goiter refers to the abnormal growth of the thyroid gland [1]. Sometimes it can extend totally or partially into the thoracic cavity and can be located in the anterior or posterior mediastinum, called intrathoracic goiter or Plongeant goiter and it can compromise mediastinal structures such as the superior vena cava and the recurrent laryngeal nerve [2,5].
The clinical manifestations vary with the thyroid function and the goiter´s size, severe compressive symptoms, dyspnea, dysphagia and cough may occur, although due to their slow and progressive growth, they can also be asymptomatic [6].
After clinical suspicion, the diagnosis is easily made with images to assess the size, extent and relationship with adjacent structures and plan the surgical approach, which is the definitive treatment in these cases [2,6].
Cases
Case 1
Female, 56 years old, hypertensive, with a history of poorly controlled amyloidosis and severe nephrotic syndrome on renal replacement therapy.
She has a goiter since she was 15 years old, without medical controls; She refers that in the last five months, rapid growth of the goiter, added dysphonia, dysphagia, dyspnea on exertion with functional class III-IV.
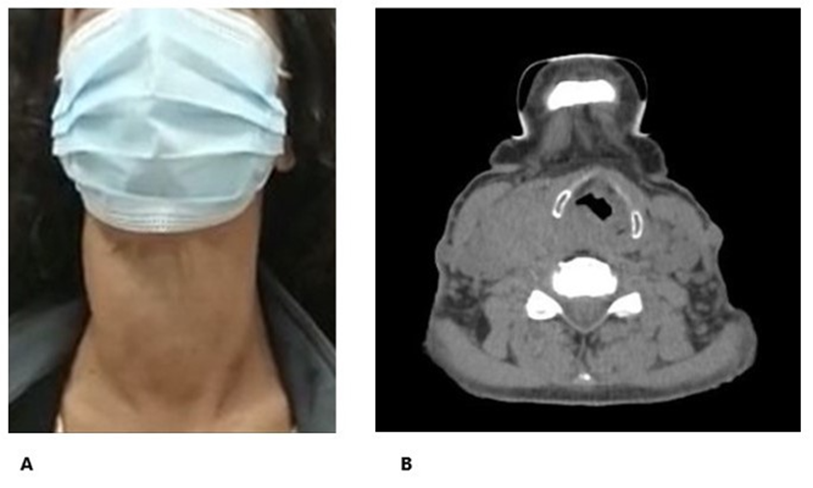
Physical examination revealed grade IV goiter, at the expense of the right lobe, firm, no lower edge palpable, positive Maranon-Pemberton (Figure 1A).
The neck ultrasound evidenced an enlarged thyroid with a volume of 72cc and a heterogeneous structure. Computed tomography scan shows enlarged thyroid at the expense of right lobule with intrathoracic extension. Total filling defect at the level of the right subclavian vein in relation to thrombosis. Visceral axis displaced to the left (Figure 1B).
In laboratory tests, she presented significant renal dysfunction (creatinine: 14,3 mg/dL), moderate anemia (Hb: 8.3 g/dL), and normal thyroid function. Given her multiple uncontrolled pathologies, altered Para clinics, it is decided that she its’ not in a surgical opportunity, she will be evaluated by her treating teams as soon as possible, to perform the surgery as quickly as possible.
Case 2
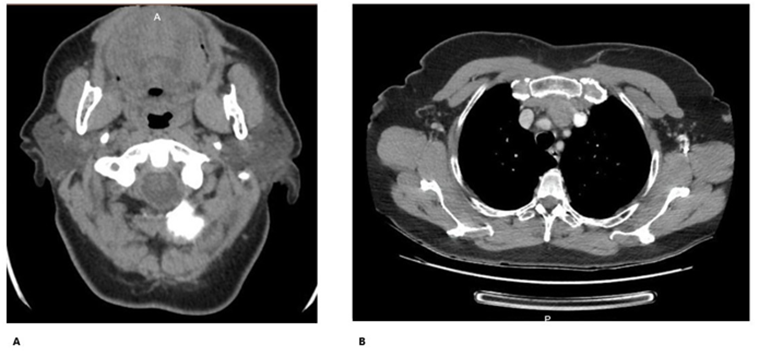
Woman, 68 years old, healthy. She presents a rapidly growing neck tumor with locoregional symptoms of 6 months' evolution. Computed tomography (Figure 2A y 2B) of the neck and chest shows a solid expansive process (71 x 54 x 90mm) that replaces the right thyroid lobe, displacing the trachea and esophagus, with a 29mm intrathoracic component that compresses without obstructing the lumen of the left brachiocephalic trunk. Small bilateral nodes.
Fine needle aspiration puncture of a 6 cm thyroid nodule: Bethesda VI.
Total thyroidectomy was performed without complications. Pathology: differentiated thyroid cancer, follicular pattern and tall cells.
In the case of thyroid cancer, with an initial intermediate risk of recurrence, radioyodo 131 (150mCi) is applied.
During follow-up: Tiroglobuline greater than 1000 ng/dl. Computed tomography: nodular lesion in the right thyroid lodge, 18x26x25mm in relation to the brachiocephalic trunk; in the thorax, adenopathic conglomerate, heterogeneous with hypodense sectors (necrosis) of 37 x 25 x 43 mm (Figure 2B). Multiple pulmonary nodules.
Given an incomplete structural response, a whole-body scintigraphy was performed that showed uptake at the base of the neck, at the retrosternal level, and at the level of both lungs. The medical team decides to perform a new surgery. At this time, the patient is undergoing preoperative evaluation.
Case 3
A 77-year-old woman with a history of chronic obstructive pulmonary disease and Parkinson's. He refers to having a goiter since childhood, three years ago he refers to its growth, adding dyspnea and dysphonia.
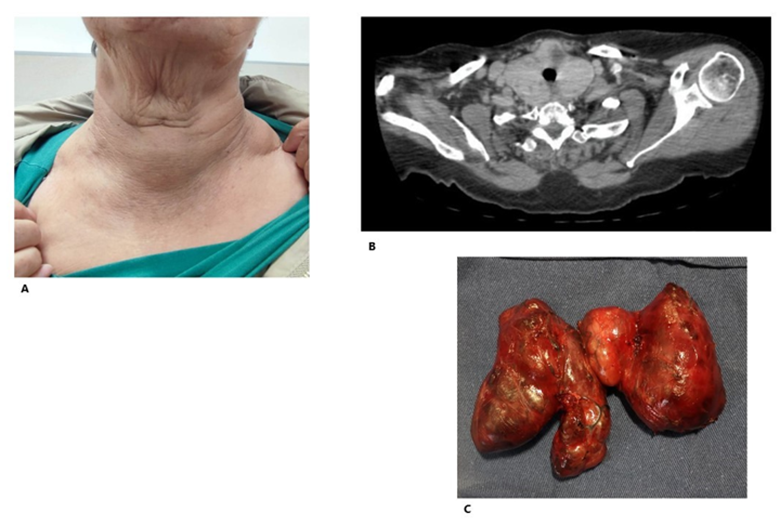
On physical examination, grade III goiter, firm, irregular elastic, non-palpable lower border (Figure 3A). Positive Maranon-Pemberton maneuver. Thyroid Eufunction.
Thyroid ultrasound: goiter 85cc, right lobe: 45cc, solid hyperechogenic nodule without vascularization (33x29x26mm). Left lobe: 40cc, solid hyperechogenic nodule (39x31x26mm). Chest computed tomography: intrathoracic extension of 40 mm, with stenosis of the tracheal lumen (Figure 3B).
Total thyroidectomy was performed without incident. (AP: multinodular goiter, without evidence of malignancy) (Figure 3C). With clear improvement in symptoms in the postoperative period.
Case 4
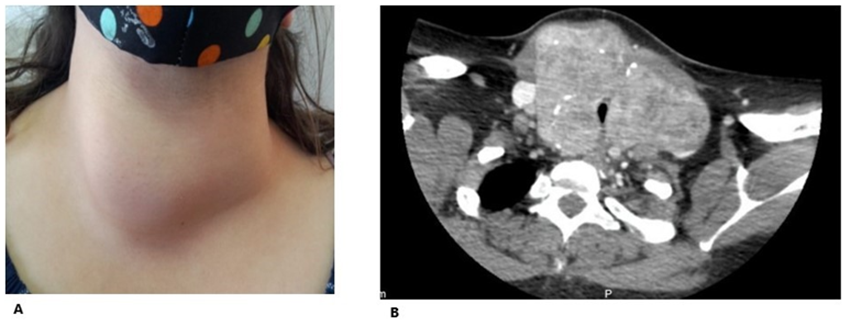
Woman, 28 years old, epileptic and with no other notable history. He presents goiter of 11 years of evolution, asymptomatic. On physical examination: grade III goiter (Figure 4A), starting in the right lobe, with no palpable lower edge. Cashew-Pemberton negative. Normal TSH.Neck ultrasound: thyroid volume of 226 cc, with a predominance of the right lobe, heterogeneous echo structure. Compression and left posterolateral displacement of the trachea (estimated diameter 6mm).
Chest and neck computed tomography: Thyroid with diffuse enlargement, predominantly in the right lobe, 75mm x 104 x 72. Narrowing of the tracheal lumen, deviation to the left. Displaces both yugulo carotid bundles laterally (Figure 4B).
Medical team and patient decide surgical treatment, total thyroidectomy. Pathology: multinodular goiter without elements of malignancy. He presented good post-surgical evolution.
Discussion
Intrathoracic goiter is the one that is partially or totally in the mediastinum and that, in hyperextension of the neck, has its lower edge at least 3 cm below the manubrium sternalis [1].
Diagnosis is made clinically and with imaging tests. The treatment of choice is surgical [2].
Its incidence is related to that of multinodular goiter; it is more frequent in endemic areas of iodine deficiency [3].
The most common location is in the anterosuperior mediastinum, followed by the posterior mediastinum with a retro tracheal or retroesophageal component [4].
It is classified into primary and secondary [5]. Primary intrathoracic goiter results from the development of ectopic thyroid tissue, the product of an abnormal migration of the thyroid primordium, it is congenital, it is truly intrathoracic, it does not present continuity with the cervical thyroid gland, it has vascularization coming from the intrathoracic vessels. It represents less than 1% [6].
Secondary intrathoracic goiter is acquired and is the most common. It arises from the cervical thyroid gland, due to its growth and descent towards the thorax, favored by its lower limit of low resistance, negative intrathoracic pressure, the downward traction produced by swallowing and the weight of the gland, its vascularization is exclusive thyroid [6].
It is more common in women (3:1 ratio), between the fifth and sixth decade of life, its main etiology is multinodular goiter, followed by follicular adenoma and Hashimoto's thyroiditis [7]. The incidence of malignancy varies between 3–16%. Its incidence increases with age, iodine deficiency and pathologies that cause elevated TSH [3].
Approximately 20-30% of cases are asymptomatic. Given the progressive growth, the symptoms appear after years of evolution [8] as it happens in all the cases presented. Usually, the only symptom is the presence of a cervical mass, they may also present symptoms secondary to compression of the intrathoracic structures, such as dyspnea, stridor, dysphagia, hoarseness, esophageal varices with digestive bleeding, superior vena cava syndrome [9].
On physical examination, most patients show a palpable neck mass, tracheal deviation, and a positive Maranon-Pemberton maneuver [6].
It is important to assess the characteristics of the tumor, adherence to deep planes, surrounding adenopathy, stony consistency, which lead to suspicion of malignancy [2,6].
The majority (as here), intrathoracic goiters are euthyroid, but they can be associated with hypothyroidism or hyperthyroidism, so it is important to carry out an anamnesis and a physical and laboratory examination [6].
The diagnosis is clinical and paraclinical, chest X-ray will show a mediastinal mass, thickening of the upper mediastinum or tracheal deviation and compression [3,5].
Contrast computed tomography scan is the examination of choice, as it provides more precise information about the relationships between intrathoracic organs and goiter, and is useful for planning the surgical approach [6,8].
The treatment of choice is surgical [5]. The choice of the type of surgery depends on the location, size and relationship of the mass with the vital structures of the mediastinum; Total thyroidectomy is the surgery of choice, since reintervention is associated with a greater number of complications [5].
Different surgical approaches can be used, depending on the extent of the goiter, cervical approach with collar incision, cervicothoracic approach (primary goiters located in the posterior mediastinum), sternotomy, thoracotomy, and thoracoscopy [1].
The most frequent post-surgical complications are hypocalcemia due to injury to the parathyroid glands, recurrent nerve injuries, bruising, bleeding, surgical wound infections, airway complications, and respiratory tract infection [3,9].
Conclusion
Intrathoracic goiter is a clinical entity with important repercussions on the patient's health, especially due to the compressive elements it produces that can cause severe obstruction of the respiratory tract. Clinical evaluation, laboratory tests and images are important to assess both the etiology, associated diseases and treatment. Total thyroidectomy by an experienced surgeon is the treatment of choice.
Thoracotomy was not required in any of our cases and there were no postoperative complications, which is a priority to maintain a good quality of life in these patients.
Conflicts of Interest
We have no conflicts of interest to disclose.
References
- Aguiar-Quevedo. (2010). Bocio intratorácico. Revisión de la literatura médica. Revista de Cirugía Española.
View at Publisher | View at Google Scholar - Madjar, D. W. (1995). Retrosternal goiter. Chest,
View at Publisher | View at Google Scholar - C.N. Foroulis, K. R. (2009). Primary intrathoracic goiter: A rare and potentially serious entity. Thyroid. Ríos, J. R. (2004). Resultados del tratamiento quirúrgico en 247 pacientes con bocio multinodular con componente intratorácico. Cir Española.
View at Publisher | View at Google Scholar - Andrade et al. (1977). A review of 128 cases of posterior mediastinal goiter. World J Surg.
View at Publisher | View at Google Scholar - Pazos, M. B. (2020). Bocio intratorácico. Revista Médica Sinergia.
View at Publisher | View at Google Scholar - Ríos, J. R. (2015). Surgical management of multinodular goiter with compression symptoms. Arch Surg.
View at Publisher | View at Google Scholar - A.R. Zambudio, J. R. (2004). Prospective study of postoperative complications after total thyroidectomy for multinodular goiters by surgeons with experience in endocrine surgery. Ann Surg.
View at Publisher | View at Google Scholar - F. Al-Mufarrej, M. (2008). Novel thoracoscopic approach to posterior mediastinal goiters: Report of two cases. J Cardiothorac Surg.
View at Publisher | View at Google Scholar
