

Research Article | DOI: https://doi.org/10.31579/2835-7957/004
Newborn Ponderal Index Centile Charts for Sri Lankan Population. – A Multicenter Study
- R S De Silvaa 1*
In-Charge Forensic Science Laboratory, Jharkhand Raksha Shakti University, Ranchi Jharkhand.
*Corresponding Author: R S De Silvaa, Registrar in Obstetrics and Gynaecology, Apeksha Hospital, Maharagama, Sri Lanka.
Citation: R S De Silvaa (2022). Newborn Ponderal Index Centile Charts for Sri Lankan Population. – A Multicenter Study. Clinical. Reviews and Case Reports.1(1); DOI:10.31579/2835-7957/004
Copyright: © 2022 R S De Silvaa, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 October 2022 | Accepted: 14 October 2022 | Published: 24 October 2022
Keywords: bioinformatics; DNA; newborn ponderal index; small for gestational age
Abstract
Introduction: Newborn Ponderal index (PI) is an anthropometric measurement that acts as an indicator of fetal growth in utero. It is calculated by dividing the birth weight (kg) by the cube of the birth length (m). Traditionally birthweight has been used for the purpose of determining the severity of growth restriction. Small for gestational age (SGA) is defined when birthweight lies under the 10th centile of the population. Many clinicians consider SGA as an equivalent to fetal growth restriction (FGR). However, it has to be appreciated that FGR is a separate entity which is defined as the failure to achieve genetic growth potential by a fetus. Thus, it has to be clearly understood that all growth restricted fetuses are not SGA while all SGA fetuses are not growth restricted. More than 40% of SGA fetuses are genetically determined to be constitutionally small and thus are generally healthy.
PI below 5th centile can be used to identify growth restricted newborns. Growth restricted neonates, irrespective of the birth weight, are vulnerable not only for short term morbidities but also for long term adverse effects such as metabolic disorders in adulthood.
Accurate identification of FGR is therefore essential for anticipation and proper management of short term and long-term complications of newborns which will lead to reduction of non- communicable metabolic disorders. Although PI centile charts are widely available for international populations, they were not available for the Sri Lankan population. Extrapolation of international PI centile charts for the Sri Lankan population may not be ideal due to socio demographic as well as genetic reasons.
Objective: To develop a reference PI centile chart for the Sri Lankan Population.
Method: A multicenter prospective cohort study was done with 3961 newborns born during the calendar year of 2014 in 02 teaching hospitals i.e. Mahamodara, Galle and Sri Jayewardenepura General Hospital, Thalapathpitiya, Nugegoda. Newborns whose gestational age was not confirmed by first trimester ultrasound scan were excluded. Gestational age at delivery of the newborn was recorded. Birth weight of the newborn was measured immediately after the initial suckling, using a digital weighing scale. Supine length was measured using an infantometer.
PI was calculated for each neonate. PI centiles were calculated from 32nd to 41st completed gestational weeks. For each gestational week 5th, 10th, 50th 90th and 95th centiles were calculated, and a centile chart was generated with the PI value pitted against the gestational age.
Results: The first ever PI reference chart for the Sri Lankan population was developed.
Conclusion: The values observed differ from international centile charts. Therefore, it will be prudent clinical practice to employ this Sri Lankan PI chart to verify antenatally diagnosed FGR as well to detect hitherto undiagnosed FGR and plan management accordingly.
Introduction
Fetal growth restriction (FGR) is one of the main causes of perinatal morbidity and mortality especially among developing countries. FGR is defined as inability to achieve the genetically determined growth potential of the fetus [1]. On the other hand, small for gestational age (SGA) means that the estimated fetal weight is below the tenth centile of the population concerned [1]. FGR and SGA are synonymously used by many authors, although they describe two interrelated yet different entities. While some newborns classified under SGA show higher perinatal morbidity and mortality, some other babies within this group can be entirely normal as they are constitutionally small and have reached the expected growth potential.
It is challenging to differentiate true FGR from SGA both antenatally and postnatally. Since the definition of SGA is straightforward, estimated fetal weight and birth weight can be used to detect SGA antenatally and postnatally respectively. However, when it comes to the diagnosis of FGR antenatally, it needs a growth trajectory of multiple scans as it relates to the fetal growth over the time.
When it comes to newborns, detection of the degree of in utero growth restriction becomes a challenge. Though birth weight can simply be used to define SGA, how the degree of FGR be defined in newborns is not well defined. Birth weight per se is not enough to determine the degree of FGR in keeping with the definition of the latter [1].
Ponderal index (PI) is widely used to detect the degree of FGR or degree of “wasting” in neonates. [2-6]. PI is an anthropometric measurement which is derived by dividing the birth weight (kg) by the cube of birth length (m). (Birth weight / Birth length 3). It is related to body mass index (BMI) in adults but more specific to detect the degree of growth restriction. PI value varies with the gestation, and it is necessary to have PI centiles for specific gestations to interpret results accurately. PI centiles charts are available internationally, but none have been developed for the Sri Lankan population. Mean neonatal anthropometry including PI differs from region to region [7]. Having a Sri Lankan PI centiles enables interpreting data of Sri Lankan neonates more accurately rather than using internationally published PI centiles.
Since FGR is linked with Poor detection of FGR appears to be an important reason behind the worldwide escalation of NCD rates in epidemic proportions, knowing the vulnerable neonates enables tailor-made lifestyle modifications to be made in order to minimize the potential harmful effects in the future.
Materials And Methods
A prospective cohort study was done in two obstetric units i.e., Unit A of Teaching Hospital Mahamodara, Galle and Ward 09 of Sri Jayewardenepura General Hospital, Nugegoda, Sri Lanka. Ethical clearance was obtained from the ethics review committee of the Faculty of Medicine, University of Ruhuna, Karapitiya, Galle, Sri Lanka. Total of 3961 neonates who were born in the calendar year of 2014 were investigated. The number of neonates included were 2788 and 1173 from Teaching hospital Mahamodara and Sri Jayewardenepura General Hospital respectively. Sequential sampling method was used. Written consent was obtained from the parents after explaining the purpose of the study and handing over an information leaflet. Inclusion criterion was all singleton pregnancies with a dating scan performed between 11-14 weeks and ended in live births. Those who consented to participate in the study were included in the study. Exclusion criteria were where written consent could not be obtained, those babies who were not followed up to the delivery in the units concerned, babies of mothers with any form of diabetes and newborns with congenital anomalies.
Birth weight was recorded by a calibrated scale which met the standards of measuring birth weight of neonates. Birth length was recorded by a standard infantometer. Both measurements were taken soon after delivery. Gestational age at delivery was recorded at the same time.
Teaching sessions were conducted to all staff involved regarding measurement of birth length to ensure correct technique and uniformity were followed in measuring birth length.
PI at birth was calculated for each neonate in the study and tabled against the gestational age at delivery. Microsoft Excel was used to construct a basic PI centile chart. Basic PI chart was modified using statistical smoothing methods to obtain a proper PI centile chart.
Results
Maternal age range was between 17 years and 42 years with a mean age of 30.2 years. Out of 3961 deliveries 2218 (55.9%) were vaginal births and 1267 (31.9%) were caesarean sections. Number of assisted vaginal deliveries was 476 (12%). Distribution of parity is given in table 1.

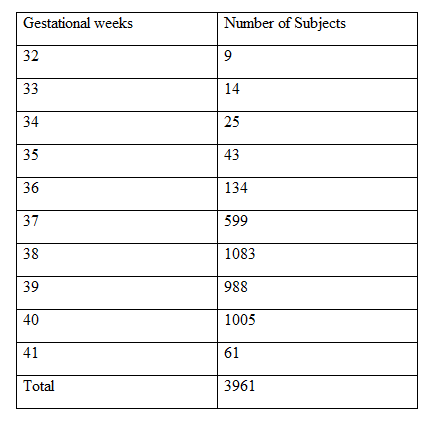
Range of gestational weeks was 32 to 41. The number of subjects corresponding to each gestational week is given in table 2.
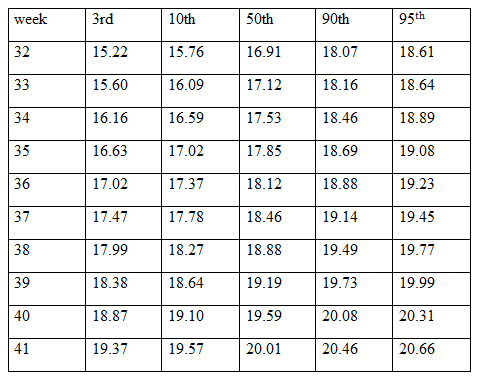
PI was calculated for each gestational age group separately. 5th, 10th, 25th,50th, 75th,90th and 95th centiles were calculated for each gestational week. PI centiles against gestational weeks is given in table 3.
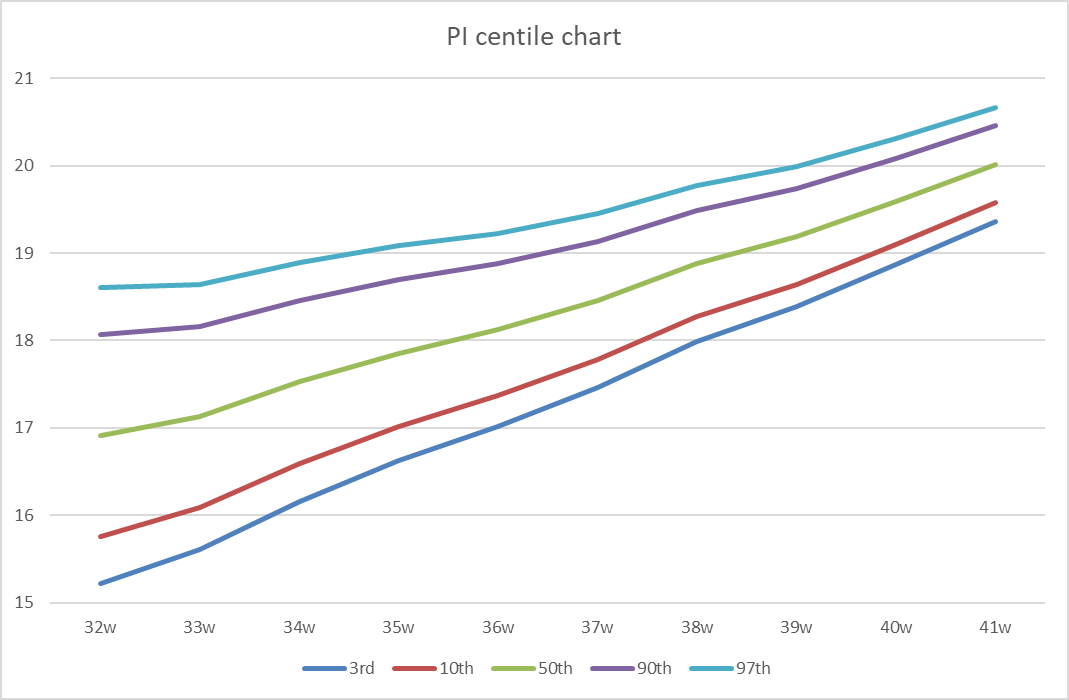
We then created a PI centile chart using PI centiles for each gestational week. Obvious outliers were excluded. It has to be taken in to account that there were limited subjects for preterm gestations. The standard deviation is high in early gestations as the numbers are low.
The PI centile chart thus generated is shown in figure 1.
Discussion
In a previous study [8], we highlighted the necessity of Sri Lankan PI centiles to make it population specific.
The two hospitals selected for the study catered for different socio economic, cultural and racial representatives of Sri Lankan population and as such, reflected a reasonable cross-sectional representation of the general Sri Lankan population.
Since birth weight alone is not adequate to determine the degree of FGR in a neonate, various parameters have been developed to this purpose. Ponderal index, skinfold thickness, mid arm circumference to occipitofrontal circumference ratio is among these parameters [9]. PI is convenient and readily reproducible among these parameters and therefore widely used.
Researchers have identified the importance of neonatal PI long since 1965. Lubchenco et al in 1965 described that “under nutrition in utero” can be recognized by PI after a study with 4706 newborns in Colorado General Hospital, USA which is now known as UC Health University of Colorado Hospital. They developed the first PI centile charts in history [10].
Later in 1971 Miller and Hassanein through their study done in University of Kansas medical Center Kansas, USA with 1437 newborns recognized that the low PI was associated with impaired fetal growth. They also emphasized that the weight alone does not successfully identify newborns with impaired fetal growth. They too developed a PI centile chart using their study population [11].
Lehingue et al has done a multicentre study in France and Belgium using 100716 subjects born between 1984 and 1988 [12] The study had a fair number of statistical elements. They applied different values for the exponent β in the formula of weight / length β to see which value predicts the best neonatal outcome. They concluded that the best prediction occurred when the exponent was 3. This in fact is the same formula used to calculate PI. They constructed neonatal PI centile charts especially, for both sexes. The study highlighted the importance of the association of low PI with poor neonatal outcome.
The largest study so far to develop PI charts was done by Landmann et al in 2004 in Germany which used 480841 subjects [13]. They developed PI charts separately for each sex and a common PI chart without considering sex. They recommended PI as a tool to differentiate symmetrical and asymmetrical FGR. They recommended their PI charts be used for the European population and highlighted that the fetal growth differs from population to population, hence the importance of referring to PI charts which are designed for a particular population. Since this study is the largest done so far to construct PI centiles, the PI chart introduced by Landmann is the widely used PI chart up to date.
The concept of fetal ponderal index (FPI) was first introduced by Vintzileos et al in 1986. They calculated estimated fetal weight (EFW) and estimated fetal length (EFL) sonographically, which then used to define FPI [14]. They then showed that FPI is comparable to neonatal PI. Later studies showed that low FPI is associated with poor perinatal outcome [15]. The concept helps spot diagnosis of FGR without recourse to serial growth trajectory. It can be of great economical advantage over serial scans which may sometimes be difficult or not feasible in some resource poor settings.
The detection of FGR in low-risk pregnancy is usually very low as the threshold of suspicion is minimal. Evidence suggests that detection rate of FGR is about 15% in low-risk pregnancies [16]. Serial growth scans are not routinely carried out in low-risk pregnancies and lead to many preventable Intra uterine deaths secondary to undetected FGR. As such, FPI will serve as a useful tool to identify FGR [17-18].
Unfortunately, studies done on FPI are scarce. A study done by Fay et al at Nepean Hospital, Penrith, New South Wales, Australia as early as 1990 analysing 2508 newborns concluded that neonates with low PI are prone to poor perinatal outcomes than neonates with low birth weight [3]. They also raised concern regarding the unavailability of PI in utero which in turn led to the development of fetal ponderal index (FPI) by them. Therefore, it was clear that the effects of FGR is not evident solely as SGA and hence a different parameter is required to assess the effects of FGR. Since then, many researches around the world emphasized that PI is a better determinant of FGR as well as a determinant of poor neonatal outcome.
Egbeyemi et al in 2018 by a Nigerian study presented FPI norms for gestations of 14 to 42. However, this study is limited by the low number of 384 subjects leading to a rather low statistical power [19].
Identifying neonates with FGR not only helps to manage neonatal complications but also helps to plan lifestyle modifications in adult life. Baker described the “Thrifty phenotype” hypothesis in which maladaptation’s that occur in fetuses under the influence of placental insufficiency can lead to adult diseases such as diabetes, hypertension, ischemic heart disease, dyslipidemia and stroke [20-22]. The basis of the hypothesis is that attempts taken by the fetus to adapt to an environment with low resources lead to its metabolism to be programmed in such a way to handle low volumes of resources. Such adaptations would not tolerate the influx of a high volume of nutritional resources experienced in later childhood and adult life. Therefore, it leads to metabolic consequences and events which ultimately lead to adult metabolic syndrome. This hypothesis also suggested that subclinical cardiac failure is apparent in FGR fetuses, and these changes will continue in adult life [22]. Some authors suggest that FGR can result in renal failure and neurodevelopment malfunctions in adult life [23].
We suggest identifying neonates with FGR and applying tailor-made lifestyle modifications that are designed to minimize the consequences of the above-mentioned metabolic challenges. Good exercise programs and healthy diet would either prevent metabolic syndrome or delay the onset in adult life. Such a tailor-made approach is not practiced in the world with regards to FGR neonates and probably explains the inability to reduce the burden of non-communicable diseases despite many interventions practiced at present.
Conclusion
Having Sri Lankan PI centiles paves the way for more research on FGR carried out in Sri Lanka. This multicenter study minimizes the potential regional variation. Large scale multicenter study including more subjects as well as earlier gestations would be the scope of future research.
More attention should be paid on research to explore the link between FGR and adult disease as complications of metabolic syndrome are becoming more common and a burden to society. For this purpose, a large scale follows up cohort studies are required. Until further research to establish the link between FGR and adult metabolic syndrome are carried out, we presently recommend early lifestyle modifications in childhood to be initiated in the neonates with low PI which most likely points to FGR.
Concept of fetal ponderal index should be explored more with regard to the spot diagnosis of FGR by a single scan. Further research is necessary as minimal studies have been performed on that concept so far. We recommend a record keeping system for the ultrasound scans performed during pregnancy for such future research.
Acknowledgments
Patients who contributed for the study and staff of Sri Jayewardenepura General Hospital and Teaching Hospital Mahamodara, Galle.
Author Contributions
HP gave the outline of the study and designed the study. RD collected data, analyzed and wrote the article. Both HP and RD proof read the article and optimized the paper.
Conflicts Of Interest
Authors don’t have conflicts of interests to specify.
References
- Royal College of Obstetricians and Gynaecologists, (2013).
View at Publisher | View at Google Scholar - P. Owen, J. Ogah and B. e. a. (2003). Bachmann,
View at Publisher | View at Google Scholar - R. A. Fay and e. a, (1991).
View at Publisher | View at Google Scholar - D. Roje, I. Banovic, and I. e. a. Tadin, (2004).
View at Publisher | View at Google Scholar - F. NILI, M. MAKIPOUR and J. MOBINI, (2003).
View at Publisher | View at Google Scholar - L. Sletner, B. Nakstad and C. Yajnik, (2013).
View at Publisher | View at Google Scholar - R. S. De Silva and H. Perera, (2021).
View at Publisher | View at Google Scholar - P. Owen and K. Khan, (1998).
View at Publisher | View at Google Scholar - L. O. Lubchenco, C. Hansman and E. Boyed, (1996).
View at Publisher | View at Google Scholar - H. Miller and K. Hassanein, (1971).
View at Publisher | View at Google Scholar - Y. Lehingue, L. Remontet, F. Munoz and N. M. Inserm, (1998).
View at Publisher | View at Google Scholar - E. LANDMAN, I. REISS, B. R. MISSELWITZ and L. GORTNER, (2006).
View at Publisher | View at Google Scholar - A. M. Vintzileos, J. G. Lodeiro and S. J. e. a. Feinstein, (1986).
View at Publisher | View at Google Scholar - G. Vilbergsson and M. Wennergren, (1992).
View at Publisher | View at Google Scholar - F. Figueras and J. Gardosi, (2011).
View at Publisher | View at Google Scholar - J. E. Lawn, S. Cousens and J. Zupan, (2005).
View at Publisher | View at Google Scholar - W. J. Ott, (2002).
View at Publisher | View at Google Scholar - O. Egbeyemi, A. Ugwu and M. Promise, (2008).
View at Publisher | View at Google Scholar - C. N. Hales and D. Barker, (2001).
View at Publisher | View at Google Scholar - D. Barker, (2001).
View at Publisher | View at Google Scholar - E. Demicheva, (2014).
View at Publisher | View at Google Scholar - E. Cosmi, T. Fanelli and S. Visentin et al, (2011).
View at Publisher | View at Google Scholar
