

Case Report | DOI: https://doi.org/10.31579/2835-7957/014
Intrapancreatic Accessory Spleen: A Diagnostic Challenge
1 Department of General Surgery, University of Health Sciences, Ankara Oncology Training and Research Hospital, Ankara, Turkey.
2 Department of Surgical Oncology, University of Health Sciences, Ankara Oncology Training and Research Hospital, Ankara, Turkey.
3 Department of Pathology, University of Health Sciences, Ankara Oncology Training and Research Hospital, Ankara, Turkey.
*Corresponding Author: G Acun, Department of General Surgery, University of Health Sciences, Ankara Oncology Training and Research Hospital, Ankara, Turkey.
Citation: Acun G., Guner E., Gulben K., Yenidunya S., (2023), Intrapancreatic Accessory Spleen: A Diagnostic Challenge. Clinical Reviews and Case Reports.2(1); DOI:10.31579/2835-7957/014
Copyright: © 2023, G Acun. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 23 February 2023 | Accepted: 08 March 2023 | Published: 16 March 2023
Keywords: intrapancreatic spleen; pancreatic tumor; accessory spleen; pancreas lesion; intra-abdominal mass
Abstract
Intrapancreatic accessory spleen (IPAS) is a rare anatomical variation and often confused with malignant tumours of the pancreas. In this case report; a 58-year-old male is presented with a several-month history of intermittent abdominal pain in the left upper quadrant. Computed tomography (CT) scan reported a hyper vascular solid lesion with a size of 20x12 mm in the pancreatic tail. A distal pancreatectomy and splenectomy were performed due to the suspicious findings on CT imaging concerning a malignant tumor and abdominal symptoms. Definitive pathological examination reported a diagnosis of IPAS in the pancreatic tail.
In spite of current researches and developing diagnostic technologies, IPAS has still a diagnostic challenge for clinicians and leads to unnecessary resections. We presented a case with IPAS who diagnosed incidentally after the pancreatic resection and wanted to take attention to this rare benign entity. It is important to keep in mind this uncommon anatomical variation for clinicians and especially surgeons, and available algorithms should be used correctly in order to prevent unnecessary resections.
Introduction
Accessory spleen (AS) is a congenital abnormality which is caused by fusion failure of splenic tissue during the fifth week of embryonic life [1, 2]. AS is often located in the peripheral area of the spleen, and the other common location is pancreatic tail [3]. Prevalence of intrapancreatic accessory spleen (IPAS) is of 1.1percentage to 3.4percentage [1]. They are frequently small and asymptomatic lesions. Dimensions of the lesions are usually about 1 cm in diameter, but sizes may range from a few millimetres to 2-3 cm [4].
Neuroendocrine neoplasms like islet-cell tumours and metastasis from renal cell carcinoma should be considered in differential diagnosis of IPAS (5). If IPAS is not combined with idiopathic thrombocytopenic purpura (ITP) and does not cause symptoms, treatment is not required [6].
However, IPAS is usually discovered incidentally after surgery for suspected cancer foci. We report a case of IPAS resected at our center.
Case Presentation
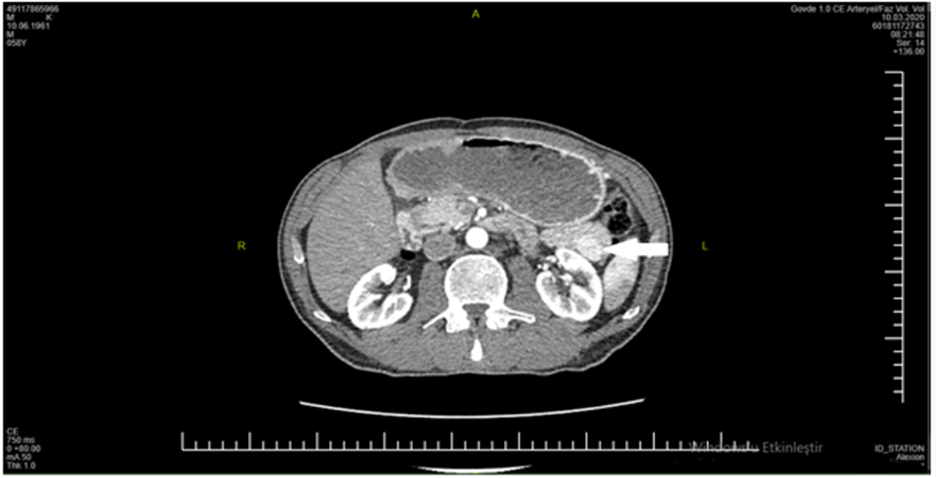
A 58-year-old male was referred to our center by detecting a mass in the pancreas tail on radiological imaging studies. He presented with abdominal pain in the left upper quadrant. He had mildly anorexia and weight loss for two months. The patient had no family history for a cancer disease. His physical examination was normal. On CT scanning, there was a hyper vascular solid and ovoid lesion with a size of 20x12 mm in the pancreatic tail (Figure 1). Tumor markers such as carcinoembryonic antigen (CEA) and carbohydrate antigen 19-9 (CA 19-9) were within normal ranges as well as the other biochemical laboratory tests.
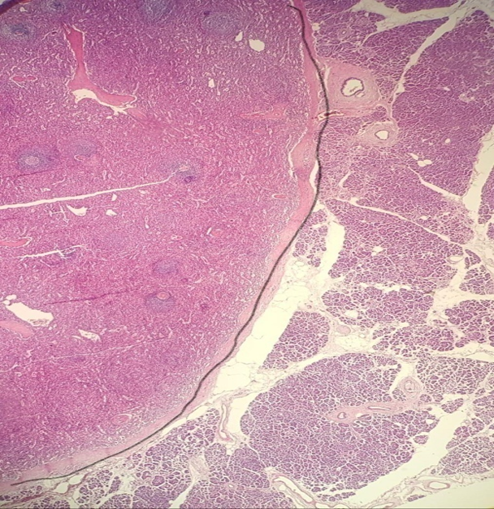
On the base of abdominal symptoms and suspicious CT findings for a cancer in the pancreatic tail, we did not need any additional imaging modalities and it was made a decision for laparotomy. During the surgical exploration, the pancreatic tissue was granular. It was palpated a mass with a size of 2 cm which was not too firm and in the form of nodularity within pancreatic tail. The patient underwent a distal pancreatectomy and splenectomy. Postoperative recovery period was uneventful for the patient, and he was discharged on the 10th postoperative day. Pathological examination of the surgical specimen was revealed a 2.2-cm accessory spleen in the tail of pancreas. IPAS was surrounded by a capsule and distinguishable from the pancreas (Figure 2 and 3).

Discussion:
AS is an anatomic variation of splenic tissue that is frequently located within the splenic hilum. Other common locations of AS are gastrosplenic ligament, splenorenal ligament, the greater momentum, the walls of the stomach or intestines, the pancreatic tail, and the mesentery. IPAS is usually an incidental finding encountered on cross-sectional imaging studies, however, making a correct diagnosis is frequently a challenge without surgery.
In a study using MEDLINE data, 46 cases of IPAS were detected incidentally [6]. In 17 of 46 patients, it was possible to establish the diagnosis without surgery. One patient was diagnosed by CT scan, three patients by endoscopic ultrasound (EUS), six patients by contrasted US and five patients by magnetic resonance imaging (MRI). They also used Tc-99m scintigraphy and immunostaining methods (CD8) to confirm the diagnosis.
CT is an important imaging method for diagnosis of this hyper vascular lesion. A study showed that unless the size of tumor reaches 3 cm, CT, MRI, or EUS could not detect lesions (6). Contrast enhancement pattern in CT is similar to hyper vascular tumours like neuroendocrine tumor. Some neuroendocrine tumours are non-functional and differential diagnosis can be difficult even with additional examinations [7]. The heterogeneous enhancement pattern during arterial phase can help to identify IPAS. This pattern results from the different blood flow rate in the white and red pulp [8, 9].
MRI is one of the other methods used in diagnosis of IPAS. Super paramagnetic iron-oxide (SIO) is a reticuloendothelial system specific contrast media which can be used to understand to what is the origin of tissue, for example liver, spleen, lymph node and bone marrow. For this reason, the use of SIO in MRI can be significant to reach the correct diagnosis. The enhancement pattern may not be similar to the spleen in small lesions, but signal intensity of IPAS can be helpful to suspect the possibility of IPAS [10].
On abdominal US, IPAS is detected as an oval shaped, homogeneous, and hypoechoic solid lesion in pancreatic tissue [11]. US is a cost-effective tool; however, it is operator-dependent and has a low sensitivity to visualize an IPAS in the pancreatic tail, particularly in obese patients.
EUS may be useful in patients who cannot be diagnosed with imaging methods [12]. In Nottingham University, EUS guided biopsy and CD8 immunostaining of splenic sinus endothelial cells identified the splenic tissue by examining the positive sections of CD8 [12.
Tc-99m can establish ectopic spleen specifically by detecting red blood cells with 90percentage accuracy [6. In a study, Tc-99m was used together with single-photon emission CT and this method could be helpful for diagnosis except minor lesions [13].
In some studies, researchers tried to make an algorithm to facilitate the preoperative distinction between IPAS and pancreatic neuroendocrine tumour. In these studies, combination diagnostic tests were recommended and EUS-guided biopsy was used for patients with cancer suspicion [1, 6].
Surgery is performed for limited indications such as symptomatic cases, hemato-oncological conditions, or ITP when the preliminary diagnosis is IPAS. Accuracy of preoperative radiological examinations are important determinant of the surgical decision. No additional imaging studies were performed for the presented case, and suspicious findings on CT scan was accepted sufficiently to make a decision for laparotomy. We also made the surgical decision together with multidisciplinary team including a radiologist for this case. According to current algorithms, a histopathological examination is not absolutely necessary to decide a surgical resection in all patients with suspected pancreatic tumor on CT scan [14]. We think that many surgeons who concern about misdiagnosis of a malignancy in the pancreas often prefer to make an operation decision as we did in this case.
Conclusion:
As imaging modalities evolve and become more common, surgeons will encounter pancreatic masses more frequently in the future. In such cases, it is important to keep in mind an AS in differential diagnosis to reduce unnecessary laparotomies.
Conflict of Interests:
None.
Funding:
None.
References
- Bing-Qi L, Xie-Qun X, Jun-Chao G. (2018). Intrapancreatic accessory spleen: A diagnostic dilemma. HPB (Oxford), 20(11):1004-1011.
View at Publisher | View at Google Scholar - Anas R, Michael H, Yousef AA, Hany M, Amanda L, et al., (2020). Diagnosis of intrapancreatic accessory spleen by endoscopic ultrasound-guided fine needle aspiration mimicking a pancreatic neoplasm: a case report and review of literature. Clin J Gastroenterol. 13(2):287-297.
View at Publisher | View at Google Scholar - Kykalos S, Machairas N, Molmenti EP, Georgios S. (2020). Intrapancreatic Accessory Spleen: Two Case Reports of a Rare Entity. Cureus. 24;12(6): e8797.
View at Publisher | View at Google Scholar - Halpert B, Alden ZA. (1964). Accessory spleens in or at the tail of the pancreas. A survey of 2,700 additional necropsies. Arch Pathol. 77:652-654.
View at Publisher | View at Google Scholar - Namita C, Gunjan S D, Chandralekha T, Prasad W. (2019). Intrapancreatic accessory spleen: an enigmatic entity. BMJ Case Rep;12: e228510
View at Publisher | View at Google Scholar - Ester O, Erez S, Joseph K, Yona G, Karen T, et.al. (2016). Pancreatic incidentaloma: Differentiating nonfunctioning pancreatic neuroendocrine tumors from intrapancreatic accessory. Endocr Pract. 22(7):773-779.
View at Publisher | View at Google Scholar - Susana M, Miguel B, Lariño N. (2016). Intrapancreatic Accessory Spleen:A Diagnosis Not to Forget!. Case Rep Gastroenterol. 13;10(3):749-754.
View at Publisher | View at Google Scholar - Kawamoto S, Johnson PT, Hall H, Cameron JL, Hruban RH, et al. (2012). Intrapancreatic accessory spleen: CT appearance and differential diagnosis. Abdom Imaging. 37:812–827.
View at Publisher | View at Google Scholar - Glazer GM, Axel L, Goldberg HI, Moss AA. (1981). Dynamic CT of the normal spleen. AJR Am J Roentgenol. 137:343–346.
View at Publisher | View at Google Scholar - Kim SH, Lee JM, Lee JY, Han JK, Choi BI. (2007). Contrastenhanced sonography of intrapancreatic accessory spleen in six patients. AJR Am J Roentgenol, 188:422–428.
View at Publisher | View at Google Scholar - Contractor U. Henderson I, Zaitoun A. (2011). Intrapancreatic accessory spleen:an important differential to consider before surgery. Human Pathology: Case Reports, 49–51
View at Publisher | View at Google Scholar - Somashekar GK, Muhannad MH, Shree GS, Tarun P, Rayburn FR. (2011). Intrapancreatic accessory spleen: investigative dilemmas and role of EUS guided FNA for diagnostic confirmation, JOP, 9;12(6):603-606.
View at Publisher | View at Google Scholar - Munk Madsen M Z, Zakarian K, Oturai PS, Hansen CP, Federspiel B, et.al. (2019). Intrapancreatic accessory spleen mimicking malignant tumor: three case reports. Acta Radiologica Open, 8(6).
View at Publisher | View at Google Scholar - Brunicardi FC. (2019). Schwartz’s principles of surgery, Mc Grawhill, 1489.
View at Publisher | View at Google Scholar
