

case report | DOI: https://doi.org/10.31579/2835-7957/056
Intraductal Papilloma with Atypical Ductal Hyperplasia of The Male Breast: A Case Report and A Brief Review
1 Department of Thyroid and Breast Surgery, Weifang Hospital of Traditional Chinese Medicine, China.
2 Medical imaging department, Weifang Hospital of Traditional Chinese Medicine, China.
*Corresponding Author: Niu Qing-Liang, Medical imaging department, Weifang Hospital of Traditional Chinese Medicine, China.
Citation: Sun Zheng, Li Long- Long, Liu Qi, Xu Chun-Hong, Li Qin, et al, (2024), Intraductal Papilloma with Atypical Ductal Hyperplasia of The Male Breast: A Case Report and A Brief Review, Clinical Reviews and Case Reports, 3(2); DOI:10.31579/2835-7957/056
Copyright: © 2024, Niu Qing-Liang. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 December 2023 | Accepted: 16 January 2024 | Published: 25 January 2024
Keywords: intraductal papilloma; atypical ductal hyperplasia; male; breast
Abstract
Intraductal papilloma (IP) is a benign tumor, which is very rare in male breast. In this report, we report a 50-year-old Chinese man who presented with a painless mass in his right breast accompanied by occasional small amount of bloody discharge. Mammography and MRI showed a subareolar nodule graded as the Breast Imaging-Reporting and Data System category 4. The patient underwent mammary gland excision through an incision along the lower edge of areola. Histopathologic examination demonstrated multiple intraductal papilloma with atypical ductal hyperplasia (ADH). There are nine cases of IP with ADH have been reported in PubMed (English language) literature until now. The most common presenting symptom is duct blood discharge. It is difficult to distinguish benign and malignant papillary lesions from invasive cancer by radiologically, should have a histopathological evaluation.
Introduction
Intraductal papilloma and atypical ductal hyperplasia are very rare conditions in male breast pathology and are rarely reported in the literature. We report a case of a 50-year-old male with a tumor that proved to be multiple intraductal papilloma with atypical ductal hyperplasia and performed a literature review.
Case Report
A 50-year-old male patient was admitted to the hospital with a painless mass of the right breast associated with occasional small amount of bloody discharge for more than 3 months. He had no history of gynecomastia due to local trauma, recent weight loss, use of anabolic steroids, or other medications. Gonadotropin levels were as follows: FSH=5.80IU/L, LH=3.82IU/L, and testosterone=5.63ng/mL. Physical examination showed a single-duct bloody discharge with tough irregular area on the outside of the right breast areola.
Ultrasound imaging of the breast revealed a 3.1cm×1.2cm×3.3cm hypoecho region with unclear boundary, irregular shape, and abundant blood flow signal(BI-RADS 4b) (Figure. 1).Mammography showed an blurred edges, uneven density, irregular dense shadows at 10 and 11 points in the right breast(BI-RADS 0) (Figure. 2).Additional magnetic resonance imaging (MRI) showed the lesions in the outer and upper quadrant of the right breast were non-mass enhancement, with segment-like distribution and unclear boundary, and the time signal intensity curve (TIC) curve was inflow type (BI-RADS 4a) (Figure. 3).
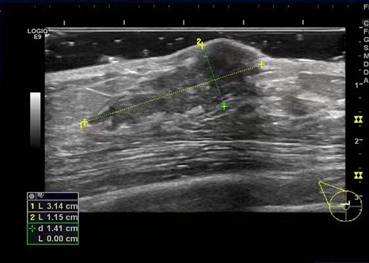

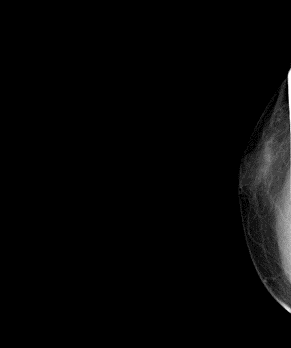
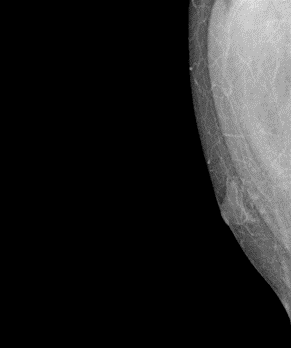
Figure 2: Mammography showing asymmetric dense shadow of right breast.
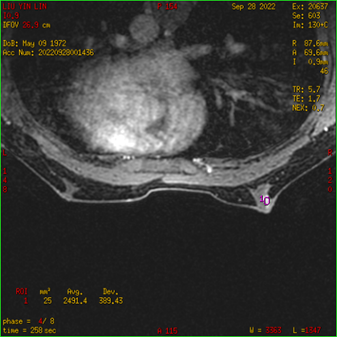
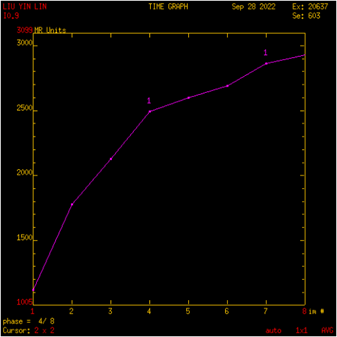
Figure 3: (A) MRI showing non mass enhancement, segmental distribution, unclear boundary. (B) TIC: Inflow type.
Preoperative core biopsy showed ductal epithelial hyperplasia without malignancy (Figure. 4). Subsequently, mammary gland excision through an incision along the lower edge of areola was performed under general anesthesia. Frozen section analysis confirmed atypical hyperplasia of duct and Nipple bottom margin negative. Preserve nipple areola complex for patients during operation. The histologic examination demonstrated multiple intraductal papilloma with atypical hyperplasia (Figures 5,6).
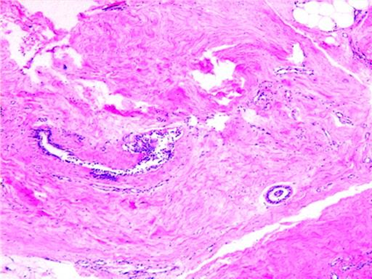
Figure 4: Partially dilated duct epithelial hyperplasia, interstitial degeneration, and hemorrhage. (H + E, ×40)
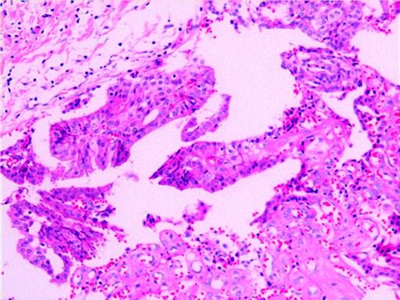
Figure 5: Multiple intraductal papilloma with atypical hyperplasia, individual ductal epithelial hyperplasia. (H + E, ×100)
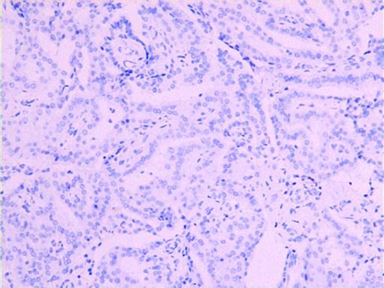
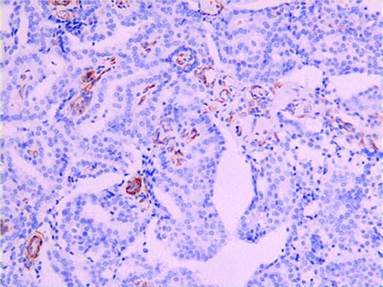
Figure 6: Immunohistochemically showing positivity of P63(A)and SMA(B).
The patient underwent mammary gland excision through an incision along the lower edge of areola. There were no postoperative complications, a good cosmetic result was achieved, and the patient was discharged home after surgery. At 3-month follow-up examination, there was no evidence of recurrence.
Discussion
Intraductal papilloma of the breast is commonly seen in 40 to 45 years old women in labor, and rarely in men 1. The actual causes of male IPs are
unclear. Although there is no clear evidence, misuse of anabolic steroids, elevated serum prolactin levels, phenothiazine treatment, and prolonged phenothiazine treatment are all triggers for the development of IP in the male breast2.Male nipple discharge is an important sign and should be evaluated with caution. [3] Breast duct endoscopy, ultrasound, mammography and MRI can assist in clinical diagnosis, but the final diagnosis depends on pathology [4].
A systematic search in PubMed revealed only 9 cases of IP in men. The clinical characteristics of patients are presented in Table 1.
| Report | Age | bloody discharge(Y/N) | ultrasonography | Mammography
| MRI | Preoperative biopsy(Y/N) | Histopathology
|
| Sara et al [5] | 71 | Y | - | - | - | N | IP |
| Tsilimigras et al[3] | 11 | Y | BI-RADS 3 | - | - | Y(FNAB) | IP |
De Vries et al. [6] | 29 | N | BI-RADS 2 | BI-RADS 3 | - | Y | IP |
| Szabo et al. [7] | 42 | Y | BI-RADS 3 | BI-RADS 3 | - | N | IP |
| IliasVagios et al. [2] | 55 | Y | BI-RADS 4 | - | - | N | IP |
| Kartik Viswanathan et al. [8] | 45 | N | - | - | - | Y | IP |
| Sushma Bharti[9] | 60 | N | - | BI-RADS 4b | - | Y(FNAB) | IP with ADH |
Durkin et al. [10] | 14 | Y | BI-RADS 4a | - | - | N | IP |
| Gaurav Anand BLA[11] | 52 | Y | BI-RADS 4 | BI-RADS 4a | - | Y | IP |
Table 1: Reported cases of intraductal papilloma in men
-: unknown.
IP:intraductal papilloma
FNAB:fine needle aspiration biopsy
ADH:Atypical ductal hyperplasia
BI-RADS:Breast Imaging‐Reporting and Data System
The median age of IP patients is 45. 66.7% (6/9) of the patients had clinical signs of bloody nipple discharge, 66.7% (6/9) of the patients underwent ultrasound examination, of which 50.0% (3/6) were assessed as BI-RADS 4, 44.4% (4/9) were assessed by mammography, and 50.0% (2/4) of the patients were classified as BI-RADS 4.55.6% (5/9) patients were diagnosed by aspiration biopsy preoperatively, including 2 cases of fine needle aspiration biopsy (FNAB) and 3 cases of core-needle biopsy. The role of FNAB in the diagnosis of benign and malignant papillary lesions remains controversial. Study of Aylin Simsir et al [12]. found that lesions displaying a papillary pattern on FNAB are nonpapillary on follow-up. Among benign processes, fibrocystic degeneration and fibroadenoma may be cytologically similar to papilloma.
Sydney et al. found that the accuracy of core biopsy in diagnosing benign papilloma was 97% [13]. In this case, we performed core-needle biopsy before operation, and 3 specimens were obtained. The pathological results failed to directly diagnose intraductal papilloma, only indicating that no malignant tumor cells were found. The reason may be insufficient specimen were obtained by preoperative aspiration biopsy.
There is no previous report on the application of MRI in male IP. The study on MRI of papillary breast diseases by Sarica et al. concluded that the main benefits of post areola imaging are its ability to show the relationship between ducts and the extension of enhanced areas14.In this case, we evaluated the lesion with MRI. A slightly longer T1 and slightly longer T2 signal lesion was seen in the upper quadrant of the right outer breast. DWI sequence showed slightly higher signal intensity, and ADC image signal was slightly reduced; After 15ml of Gd-DTPA was injected intravenously, the scanning showed that the lesions in the upper quadrant outside the right breast were non mass enhanced, distributed in segments, with unclear boundaries, and the larger slice area was about 1.4 × 1.8 × 1.2cm, TIC curve is inflow type.
Based on the patient's imaging evaluation and preoperative pathological results, we finally prepared the mammary gland excision for the patient. At the same time, according to the frozen section during the operation, we ensured that the bottom cutting edge of the nipple and areola was negative while retaining the patient's nipple and areola complex. There were no complications and the cosmetic effect was good.
Conclusion
Male IP is extremely rare, and bloody nipple discharge is the most common clinical presentation. Core-needle biopsy is helpful for preoperative diagnosis, and breast MRI evaluation can be used to determine surgical treatment regimen.
References
- Emily T, Thomas F, Peter F. (2011). Enlarging unilateral breast mass in an adolescent male: an unusual presentation of intraductal papilloma [J]. J of Pediat Surg, 46(1): 33-35.
View at Publisher | View at Google Scholar - Ilias Vagios, Aphrodite Nonni, Aliki Liakea. (2019). Intraductal papilloma of the male breast: a case report and review of the literature. Journal of Surgical Case Reports.
View at Publisher | View at Google Scholar - Tsilimigras,Ioannis Ntanasis, (2017). Stathopoulos ·Intraductal papilloma of the breast in an 11-year-old male patient: a case report. Pediatr Surg Int 33(6):727-730.
View at Publisher | View at Google Scholar - Adibelli ZH, Oztekin O, Gunhan-Bilgen I, et al. (2010). Imaging characteristics of male breast disease. Breast J. 16(5): 510-518.
View at Publisher | View at Google Scholar - Sara AS, Gottfried MR. (1987). Benign papilloma of the male breast following chronic phenothiazine therapy. Am J Clin Pathol ,87:649–650.
View at Publisher | View at Google Scholar - De Vries FE, Walter AW, Vrouenraets BC. (2016). Intraductal papilloma of the male breast. J Surg Case Rep 2016,2:1–2.
View at Publisher | View at Google Scholar - Szabo BK, Wilczek B, Saracco A, Szakos A, Bone B. (2003). Solitary intraductal papilloma of the male breast: diagnostic value of galactography. Breast J ,9:330–331.
View at Publisher | View at Google Scholar - Kartik Viswanathan, Brian McMillen, Esther Cheng. (2017). Juvenile Papillomatosis (Swiss-Cheese Disease) of Breast in an Adult Male with Sequential Diagnoses of Ipsilateral Intraductal, Invasive, and Widely Metastatic Carcinoma: A Case Report and Review of the Disease in Males. International Journal of Surgical Pathology, 25(6) :536–542.
View at Publisher | View at Google Scholar - Sushma Bharti, Jyotsna Naresh Bharti, Jeewan Ram Vishnoi. (2021). A rare case of intraductal papilloma with atypical ductal hyperplasia in a male breast: A pathological diagnosis. Gan To Kagaku Ryoho , 27(3).
View at Publisher | View at Google Scholar - Durkin ET, Warner TF, Nichol PF. (2011). Enlarging unilateral breast mass in an adolescent male: an unusual presentation of intraductal papilloma. J Pediatr Surg 46: e33–e35.
View at Publisher | View at Google Scholar - Gaurav A, Al-Khalisi N, Dauod A, Soheila H, Lewis T. (2018). Rare case of male breast intraductal papilloma progressing to invasive ductal carcinoma: a radiologic-pathologic correlation. Radiol Case Rep ,13:602–605.
View at Publisher | View at Google Scholar - Aylin Simsir, Jerry Waisman, Kim Thorner. (2003). Mammary Lesions Diagnosed as “Papillary” by Aspiration Biopsy 70 Cases with Follow-Up. Cancer Cytopathology, 99:156–165.
View at Publisher | View at Google Scholar - Sydnor MK, Wilson JD, Hijaz TA, Massey HD, Shaw de Paredes ES. (2006). Underestimation of the presence of breast carcinoma in papillary lesions initially diagnosed at core-needle biopsy. Radiology ,242:58–62.
View at Publisher | View at Google Scholar - Sarica O, Uluc F, Tasmali D. (2014). Magnetic resonance imaging features of papillary breast lesions. Eur J Radiol, 83:524–530.
View at Publisher | View at Google Scholar
