

Case Report | DOI: https://doi.org/10.31579/2835-7957/011
Entrance of Transverse Colon Volvulus into the Diaphragm Defect: A Case Report
1 Department of Surgery, School of Medicine, Kermanshah University of Medical Sciences, Kermanshah, Iran
2 Student Research Committee, Faculty of Medicine, Shahed University, Tehran, Iran.
*Corresponding Author: Mohammad Hossein Golezar, Student Research Committee, Faculty of Medicine, Shahed University, Tehran, Iran.
Citation: Navid R. Zarei, Mohammad H. Golezar, (2023), Intrapancreatic Accessory Spleen: A Diagnostic Challenge, Clinical Reviews and Case Reports, 2(1); DOI:10.31579/2835-7957/011
Copyright: © 2023, Mohammad Hossein Golezar. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 19 January 2023 | Accepted: 31 January 2023 | Published: 10 February 2023
Keywords: diaphragmatic hernia; colonic volvulus; colectomy; case report
Abstract
Background: Colonic volvulus is an uncommon yet clinically important condition. It can occur in different locations; however, transverse colon and splenic flexure are rarely involved. We hereby present a 62-year-old man with a rare condition of herniation of transverse colon and splenic flexure within the chest cavity.
Case presentation: A 62-year-old man was admitted to our center, a teaching hospital in Iran, complaining about three-day abdominal pain, anorexia, constipation, and abdominal distention. He was intellectually disabled and had a previous history of chronic constipation. The imaging studies showed the bowel loops herniated into the thoracic cavity. A laparotomy procedure was performed. The twisted transverse colon and splenic flexure were present in the left hemithorax. Total colectomy and ileostomy were performed and the diaphragmatic defect was repaired.
Conclusion: This work aimed to raise attention to the rare condition of concurrent diaphragmatic hernia and colonic volvulus. The diaphragmatic hernia can be a life-threatening condition per se. If it is accompanied by intestinal volvulus in rare cases, it creates a pressing condition. More studies are required to explain the etiology of this potentially fatal condition.
Introduction
The word volvulus comes from the Latin word Volver meaning to roll. This term is used to describe the twisting of a segment of the digestive tract [1]. Intestinal volvulus may occur in the small bowel or colon. In adult individuals, colonic volvulus is more frequent [2]. Volvulus may occur in any mobile segment of the colon. The sigmoid has the highest frequency followed by the cecum, transverse colon, and splenic flexure which is involved in only 1percentage of cases [3]. If the treatment is delayed, colonic volvulus can reduce the affected segment’s blood flow, resulting in ischemia, gangrene, perforation, and mortality [4]. Diaphragmatic hernia, which can be congenital or acquired, is a herniation of abdominal organs within the chest cavity throughout a defect on the diaphragm [5]. We hereby present a rare case of transverse and splenic flexure volvulus which was herniated within the thoracic cavity.
Case presentation
A 62-year-old man was admitted to the Surgery Department of a teaching
hospital in Kermanshah, Iran, complaining about three-day abdominal pain, anorexia, constipation, and abdominal distention which increased the night before the admission. The patient's abdominal pain was persistent, not positional, and not radiating. He mentioned consuming castor oil to improve constipation but it was not beneficial. He did not experience nausea/vomiting, fever, or change in bowel habits before current symptoms. The patient had an intellectual disability so his brother participated in the process of history taking. He had a history of colonoscopy six years before admission due to chronic constipation. The drug history and family history were unremarkable. On the physical examination, he looked unwell but his vital signs were within the normal range. Mild spinal kyphosis was observed. On the left side, the breath sounds were decreased. The abdomen was distended but not tender to palpitation. The abdominal percussion produced a tympanic note. Other parts of the examination were normal. The laboratory results revealed neutrophilia, increased creatinine, and respiratory acidosis (Table 1).
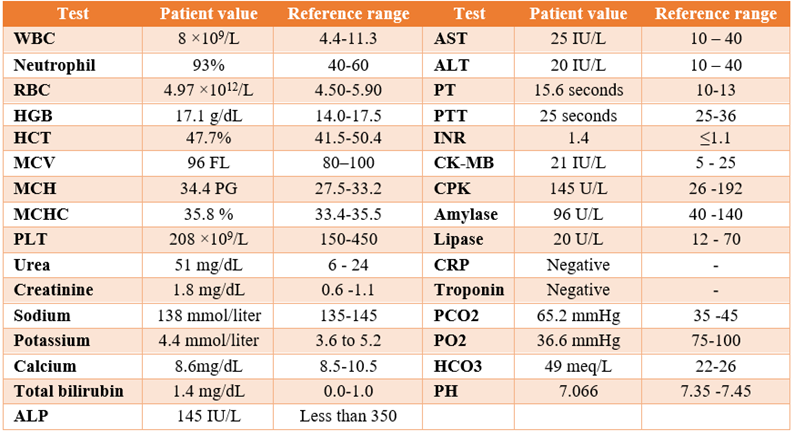
WBC= white blood cell; RBC= red blood cell; HGB= hemoglobin; HCT= hematocrit; MCV= mean corpuscular volume; MCH = mean corpuscular hemoglobin; MCHC = mean corpuscular hemoglobin concentration; PLT = platelet; ALP= alkaline phosphatase; AST= aspartate aminotransferase; ALT= alanine aminotransferase; PT= prothrombin time; PTT= partial thromboplastin time; INR= international normalized ratio; CK-MB= creatine kinase-MB; CPK= creatine phosphokinase; CRP= C-reactive protein; PCO2= partial pressure of carbon dioxide; PO2= partial pressure of oxygen; HCO3= bicarbonate.
Chest and abdominopelvic radiographs were acquired (Figure 1).
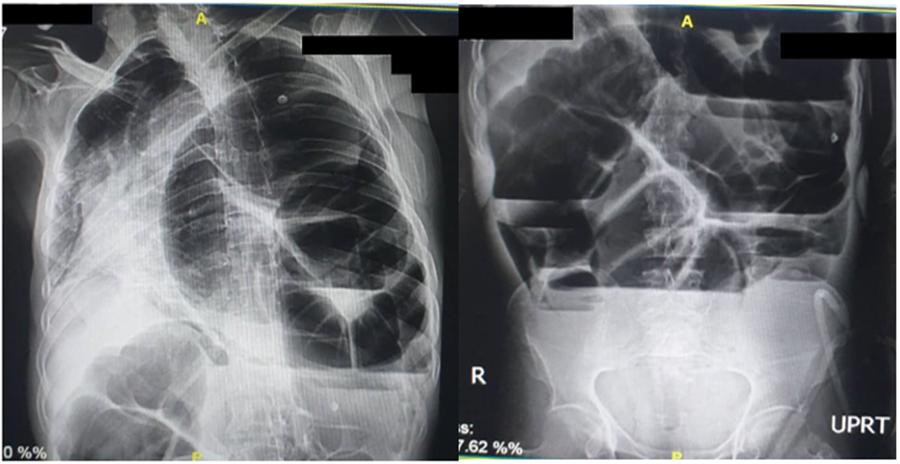
A non-contrast computerized tomography was performed and reported as follows: A large diaphragmatic defect was seen on the left side. The colon and mesentery herniated into the thoracic cavity, causing severe cardiac and mediastinal shift and left lung collapse. The colon is dilated (diameter =130 mm). The loops of the small intestine are dilated (maximum diameter =45 mm). Two areas of whirlpool signs were seen which may be due to recent surgery or volvulus. A segment of the colon is collapsed. Considering the clinical picture and para-clinical findings, the diagnosis of herniation of colonic volvulus within the chest cavity through a diaphragmatic defect was made. The patient was transferred to the operating room. Under general anesthesia in a supine position, a laparotomy with a midline incision was performed. The twisted transverse colon and splenic flexure were present in the left hemithorax (Figure 2).
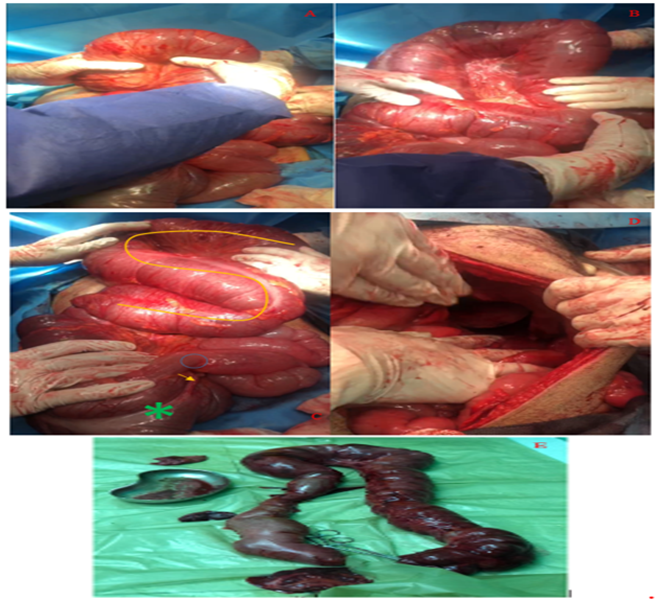
The loops of intestine were dilated. The twisted transverse colon which looked elongated was removed from diaphragmatic defect and untwisted by counterclockwise rotation. The gallbladder adherence to the colon was detached. Total colectomy and ileostomy were performed and a mucous fistula was constructed. The hernia sack was removed. The diaphragmatic defect was repaired with a dual mesh due to its large size. A chest tube was inserted and the patient was transferred to the recovery room and then the surgical intensive care unit. The patient made an uneventful postoperative recovery.
Discussion
The etiology of colon volvulus is multifactorial. Long-term constipation, high fiber foods intake, repeated use of laxatives, history of laparotomy procedure, and anatomic predisposition are some causes seen in all types of colonic volvulus [3]. Risk factors for transverse colon volvulus are distal obstruction or chronic constipation, elongation and redundancy of the colon, the narrowing of the mesenteric attachments, absence or malfixation of the mesenteries, and a fixed point around which the intestine can roll. Predisposing factors for splenic flexure volvulus are constipation and previous abdominal surgery [6]. As mentioned before, the present case had a history of chronic constipation which was a risk factor for colonic volvulus. Colonic volvulus is responsible for 3.4percentage to 50percentage of all cases of bowel obstructions in different regions [4]. The classic volvulus patient is an old, institutionalized person who is taking psychotropic medications that leads to chronic constipation [3]. Transverse and splenic flexure volvulus manifest with symptoms similar to large bowel obstruction including abdominal pain, nausea/vomiting, and constipation which can be acute or chronic [6]. The present patient was old and intellectually disabled with typical symptoms of bowel obstruction so the clinical picture was strongly in favor of colonic volvulus. Abdominopelvic computerized tomography is the method of choice in the diagnosis of volvulus [3]. Which was diagnostic in the present case. The therapeutic approach to volvulus depends on the segment involved, clinical picture, and initial para-clinical results. In complicated forms, surgery must be performed immediately irrespective of location [3]. What made this case more complex was the concurrent occurrence of diaphragmatic hernia. Congenital diaphragmatic hernia is a rare developmental deficiency of the diaphragm divided into four types: Bochdalek, Morgagni, hiatal hernia, and septum transversum defect. Bochdalek’s hernia (posterolateral) is the most frequent type [5]. Several genetic disorders have been found to cause intellectual disability and congenital diaphragmatic hernia [7]. A congenital defect may remain undiagnosed if no herniation of the abdominal structures into the thoracic cavity occurs [8]. On the other hand, acquired diaphragmatic hernias are generally traumatic [9]. In the present case, no obvious history of trauma was reported. Regarding the intellectual disability, it may be concluded that the patient had an undiagnosed congenital hernia. Colonic volvulus accompanied by diaphragmatic hernia is rarely described in the literature. Badak et al. reported a similar case; A 32-year-old man with a history of intellectual disability was admitted due to constipation and abdominal swelling. He had a previous history of sigmoid volvulus. The patient was finally diagnosed with giant recurrent sigmoid volvulus accompanied by a diaphragmatic hernia [10]. Toliczenko-Bernatowicz et al. reported a girl with a congenital diaphragmatic defect. Following an epigastrium trauma, herniation of the abdominal organs into the thoracic cavity and subsequent volvulus occurred [8]. Boumarah et al. reported an elderly with a history of hydatid cyst presenting with respiratory and abdominal symptoms for several months. Further investigations led to the diagnosis of a diaphragmatic defect with herniation of bowel loops within the thoracic cavity [11].
Conclusion
This case was presented to raise attention to a rare case of concurrent diaphragmatic hernia and colonic volvulus. Data are scarce on this simultaneity. More studies are required to explain the characteristics of this rare yet potentially fatal condition.
Acknowledgment:
We thank the patient for his informed consent to publish the case report.
Conflict of Interests:
None
Informed Consent:
A written informed consent was obtained from the patient.
Funding:
None
References
- Bauman ZM, Evans CH. (2018). Volvulus. Surgical Clinics. 98(5):973-993.
View at Publisher | View at Google Scholar - Kapadia MR. (2017). Volvulus of the small bowel and colon. Clinics in colon and rectal surgery. 30(01):040-045.
View at Publisher | View at Google Scholar - Perrot L, Fohlen A, Alves A, Lubrano J. (2016). Management of the colonic volvulus in 2016. Journal of Visceral Surgery. 153(3):183-192.
View at Publisher | View at Google Scholar - Halabi WJ, Jafari MD, Kang CY, Nguyen VQ, Carmichael JC, et al. (2014). Colonic volvulus in the United States: trends, outcomes, and predictors of mortality. Annals of surgery. 259(2):293-301.
View at Publisher | View at Google Scholar - Eren S, Çiriş F. (2005). Diaphragmatic hernia: diagnostic approaches with review of the literature. European journal of radiology. 54(3):448-459.
View at Publisher | View at Google Scholar - Gingold D, Murrell Z. (2012). Management of colonic volvulus. Clinics in colon and rectal surgery. 25(04):236-244.
View at Publisher | View at Google Scholar - Pober B. (2008). Genetic aspects of human congenital diaphragmatic hernia. Clinical genetics. 74(1):1-15.
View at Publisher | View at Google Scholar - Toliczenko-Bernatowicz D, Dębek W, Matuszczak E. (2016). Colon volvulus displaced into the chest–right-sided posttraumatic hernia or congenital malformation? Kardiochirurgia i Torakochirurgia Polska= Polish Journal of Cardio-Thoracic Surgery. 13(2):159.
View at Publisher | View at Google Scholar - Gupta S, Kaur Bali R, Das K, Sisodia A, Dewan R, et al. (2011). Rare presentation of spontaneous acquired diaphragmatic hernia. Indian Journal of Chest Diseases and Allied Sciences. 53(2):117.
View at Publisher | View at Google Scholar - Badak B, Aslaner E, Gambarov N. (2020). Giant relapse sigmoid volvulus: case report. Galician medical journal. 27(2):E202023.
View at Publisher | View at Google Scholar - Boumarah D, Alsinan A, Alothman O, AlDandan O, Alshomimi S. (2021). Acquired right-sided diaphragmatic hernia in a patient with retroperitoneal hydatidosis: a case report and review of the literature. Journal of Medical Case Reports. 15(1):320.
View at Publisher | View at Google Scholar
