

Review Article | DOI: https://doi.org/10.31579/2835-7957/031
Diabetes in Childhood: An Overview of Etiology, Analysis, and Management
- Rehan Haider *
Riggs Pharmaceuticals Karachi, Department of Pharmacy University of Karachi (Pakistan)
*Corresponding Author: Rehan Haider, Riggs Pharmaceuticals Karachi, Department of Pharmacy University of Karachi (Pakistan)
Citation: Rehan Haider (2023), Diabetes in Childhood: An Overview of Etiology, Analysis, And Management, Clinical Reviews and Case Reports, 2(5); DOI:10.31579/2835-7957/031
Copyright: © 2023, L. Barakat. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 21 July 2023 | Accepted: 25 August 2023 | Published: 05 September 2023
Keywords: protection; diabetes mellitus; childhood diabetes
Abstract
Diabetes mellitus in early life is a persistent metabolic ailment characterized by hyperglycemia due to impaired insulin production, usage, or both. This evaluation offers a comprehensive examination of the etiology, prognosis, and management of diabetes in the pediatric population. The growing prevalence of early-life diabetes globally underscores the significance of statistics on the complicated nature of sickness and the stressful situations it poses to affected human beings and their households. Etiology: Type 1 diabetes (T1D) and type 2 diabetes (T2D) are the most common office diseases among youth. T1D, often identified in early life, arises from an autoimmune reaction that ends with the destruction of pancreatic beta cells, resulting in insulin deficiency. Early-life genetic susceptibility, environmental elements, and an intricate interplay of immune and metabolic pathways contribute to the development of both types of diabetes. The diagnosis of youth diabetes consists of a careful evaluation of symptoms, blood glucose titers, and specific diagnostic standards. Symptoms may additionally encompass unusual urination, excessive thirst, unexplained weight reduction, and fatigue. Fasting and random blood glucose ranges, oral glucose tolerance tests, and HbA1c measurements are all useful tools for confirming the analysis and distinguishing T1D from T2D. Manipulated powerful control of adolescent diabetes by targeting the accumulation of glycemic manipulation while minimizing the danger of acute and chronic complications. Treatment strategies encompass insulin remedies for T1D, with several regimens tailored to men’s or women's desires. For T2D, lifestyle modifications concerning a balanced food plan and everyday physical activity are crucial additives for management, with some instances requiring oral hypoglycemic agents or insulin.
Challenges: coping with diabetes in early life offers particular demanding situations, including the desire for constant blood glucose monitoring, the functional impact on the children's psychosocial development, and the burden on caregivers. college settings require collaboration among healthcare experts, educators, and households to make certain ultimate diabetes manipulation and the kid's Key
Introduction
Introduction
The spectrum of diabetes in children
In Europe and North America, one in 300 children developed diabetes by the age of 20 years. While the rates are lower elsewhere, there are an estimated 700 000 children with diabetes worldwide
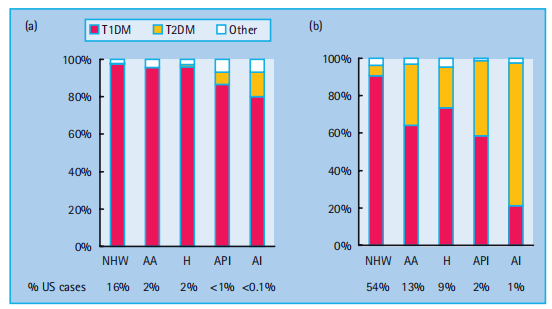
and 100 000 new cases are diagnosed annually. Diabetes is a heterogeneous disease at any age. Newborn babies and infants rarely. develop the disease (1 in 250 000 in those younger than 6 months) and its etiology is not autoimmune but is usually monogenic. From 9 months to 10 years of age, almost all diabetes cases are caused by islet autoimmunity. Type 1a (autoimmune) diabetes mellitus (T1aDM) accounts for more than 90% of the cases among older children of European ancestry; however, in other ethnic groups, 20–70% of older children may have type 2 diabetes mellitus (T2DM; Figure 51.1).
With the increasing prevalence of obesity in the general population, a significant proportion of children with T1aDM present with a phenotype that masquerades as T2DM. Measurement of autoantibodies to insulin, GAD 65, IA - 2, and ZnT8 at diagnosis, C peptide after the initial metabolic stabilization, and HLA-DR and DQ typing may be necessary to evaluate appropriate long-term treatment. This observation focused on the practical elements of the control of T1aDM in youngsters. The epidemiology and etiology of T1aDM are a result of the interplay between genetic and environmental elements. The preliminary step, the development of islet autoimmunity, marked by the presence of islet autoantibodies, is assumed to be pushed by using one or more environmental triggers [1]. Over the past 40 years, the prevalence of T1DM in youth has increased by 3 – 5% annually (Figure 51.2).
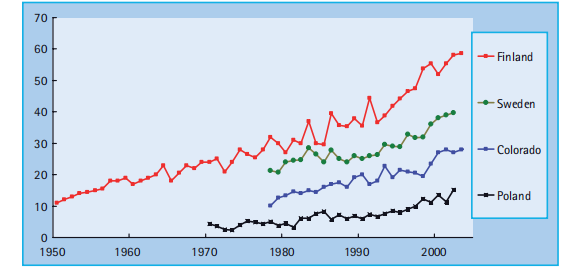
Figure 51.2 Incidence of T1DM has been rising about 3 – 5% per year.
Elimination of the environmental cause(s) chargeable for this epidemic will be the most efficient
Figure 51.1 Type - specific proportions of prevalent cases of diabetes in the US population, according to age group (a, 0 – 9 years; b, 10 – 19 years) and race/ ethnicity. AA, African American; AI, American Indian; API, Asian/Pacififi c Islander; H, Hispanic; NHW, Non - Hispanic White. Adapted from SEARCH for Diabetes in Youth Study, 2001 [30]. technique to number one prevention; however, there is a lack of consensus about which environmental factors initiate and promote islet autoimmunity. Efforts to prevent T1DM have recently been reviewed elsewhere [2]. After the initiation of islet autoimmunity, most patients have a long preclinical period, which offers an opportunity for secondary prevention of progression to clinical diabetes. The presence of more than one of the autoantibodies combined with susceptibility to HLA-DR and DQ genotypes identified those at high risk of developing diabetes. There may be a " point of no return " in the autoimmune destruction of islets, rendering some interventions effective only at the earlier stages of the process. Once tolerance is broken down to more than one islet auto antigen, most individuals progress to diabetes within 10 years. A period of mild asymptomatic hyperglycemia, detectable by oral glucose tolerance testing (OGTT) [3] or HbA 1c [4],
may precede overt insulin dependence over months or years among persons with islet autoantibodies. Intervention at this " daily comic " stage
may also theoretically preserve endogenous insulin secretion and prevent acute and long-term complications of T1DM. Preservation or regaining of residual insulin secretion after the diagnosis of diabetes might also help, but the immuno gold ovulatory agents used so far in tertiary prevention may carry unacceptable long-term risks.
Manifestation, diagnosis, and initial treatment
Clinical presentation and diagnosis
The cardinal symptoms at the time of diabetes diagnosis include polyuria (96% of children, often with nocturia or bed wetting), polydipsia, weight loss (61%), and fatigue [5]. The classic presentation
of diabetic ketoacidosis (DKA) in a thin dehydrated child with Kussmaul's breathing, abdominal pain, vomiting, and impaired neurologic status affects fewer than 30% of cases presenting in
developed countries [5,6]. With the increasing community recognition of diabetes, most children present with milder hyperglycemia of shorter duration; however, 75% of the children (63%
below age 5) had symptoms for more than two weeks, suggesting that the diagnosis could be made earlier in many cases. A young child may have a less specific presentation, for example
with vomiting or rapid breathing during infection. Diabetes should always be considered in ill children. Urine or blood testing for glucose and ketones leads to an early diagnosis and may prevent DKA and hospitalization. Nearly all patients admitted with severe DKA were seen hours or days earlier by healthcare providers who missed the diagnosis. While most children do not require intravenous fluids or insulin infusion for diabetes diagnosis, many are hospitalized for a few days. These hospitalizations can be avoided if safe outpatient alternatives and adequate reimbursement exist for this initial care. For instance, the availability of outpatient care at the center has helped decrease hospitalization at diagnosis from 88% in 1978 – 1982 to 46% in 1998 – 2001, with the proportion of hospitalizations secondary to DKA increasing from 44% to 63% [6]. The diagnostic criteria are the same in children and adults; however, most children are quite symptomatic and dominant extensive workups. In a symptomatic child, plasma glucose ≥ 11.1 mmol/L (200 mg/dL) at any time of day, without regard to time since the last meal, or fasting plasma
glucose ≥ 7.0 mmol/L (126 mg/dL) was considered diagnostic. Blood glucose results obtained using a glucose meter should be immediately confirmed in the laboratory before the initiation of insulin treatment. By contrast, if marked hyperglycemia and blood or urinary ketones are present, treatment is urgent; waiting another day to confirm the diagnosis may be dangerous if DKA is allowed to
develop. In a good child, the diagnosis must not be based on a single plasma glucose test or borderline results obtained using a gluco meter. In such cases, the authors check the HbA 1c level;
If this is normal, further monitoring of fasting and/or 2-hour postprandial blood glucose is recommended for several days. In children progressing to overt diabetes, hyperglycemia after dinner
is usually the initial abnormality detectable by self-monitoring blood glucose at home. OGTT should not be performed if fasting, random, or post-prandial criteria are met as it is unnecessary, and
Excessive hyperglycemia can result. Hyperglycemia detected incidentally or during acute infection, trauma, or other illnesses may be transient, especially if the typical symptoms of diabetes are absent or equivocal. Children with Transient hyperglycemia may be more likely to develop diabetes, but the reported progression rates vary from 0 to 32%. Testing for islets and autoantibodies help to rule out diabetes in cases with mild presentation; however, it is important to consider that the quality of commercial assays for islet autoantibodies varies widely, and testing for at least three autoantibodies (insulin, GAD 65 and IA - 2) provides an 80% predictive value.
Impaired glucose tolerance (IGT) and impaired fasting glucose (IFG) may also be detected in children with islet autoimmunity that progresses to overt diabetes [3]. OGTT is rarely needed in prepubertal children, except to reassure the family that metabolic decompensation is not imminent. In older children, especially obese teenagers with equivocal symptoms, OGTT may play a role in the early diagnosis of T2DM, IGT, and IFG.
Diabetic ketoacidosis
The clinical presentation of DKA includes abdominal pain, nausea vomiting, and vomiting which can mimic vomiting acute abdomen. The patients are mild to moderately dehydrated (5 – 10%) and may have Kussmaul's respiration became progressively somnolent and obtunded. DKA results from an absolute or relative deficiency of circulating insulin and a corresponding increase in the levels of counter-regulatory hormones such as catecholamines, cortisol, glucagon, and growth hormone. This combination leads to a catabolic state, with increased glucose production in the liver and kidneys, increased lipolysis, ketogenesis with ketonemia, and metabolic acidosis. Absolute insulin deficiency occurs in patients with previously undiagnosed T1DM or established patients with the omission of or inadequate insulin regimens. Relative insulin deficiency occurs during acute illness and stress if the increase in counter-regulatory hormones is not balanced by an appropriate increase in the insulin dosage. The severity of DKA was categorized according to the degree of acidosis.
• Mild: venous pH 7.2 – 7.3 or bicarbonate < 15>
• Moderate: venous pH 7.1 – 7.2 or bicarbonate < 10>
• Severe: venous pH < 7>
Diabetic ketoacidosis at diagnosis of diabetes In the USA and patients younger than 20 years with a clinical diagnosis of T1DM and T2DM presented with DKA in 29% and 10% of the cases, respectively [6]. In Europe, the rates of T1DM cases ranged from 15% to 67%, correlating inversely with the local incidence of T1DM [7]. DKA is more often found among younger children and children with lower socioeconomic status who encounter barriers to accessing medical care [6]. Intensive community intervention to raise awareness of the signs and symptoms of childhood diabetes among schoolteachers and primary care providers may help to reduce the prevalence of DKA at diagnosis [8]. Diabetic ketoacidosis in established patients in a large cohort of children with established T1DM, on average, 8 patients per 100 developed DKA every year [9]; however, nearly 60% of DKA episodes occurred in 5% of children with recurrent events. Recurrent DKA was predicted by poor metabolic control, previous episodes of DKA, psychiatric and eating disorders, difficult family or social circumstances, and limited access to medical care. Treatment of ketoacidosis Hydration status should be assessed, and fluid deficit and osmolality should be calculated to guide fluid and electrolyte replacement. Serum electrolytes, glucose, blood urea nitrogen (BUN), creatinine, calcium, magnesium, phosphorous, and blood gas testing should be repeated every 2 – 4 h or more frequently in severe cases. The calculations are as follows:
Anion gap Na Cl HCO =−+ () 3 Corrected Na = measured Na + [(plasma glucose – 100 mg/dL) (1.6)/100]
Serum osmolality = 2(Na + K) + glucose/18 + BUN/2.8 (mOsm/L) Patients with DKA have a 5 – 10
Research Method:
The research became performed with the use of a blended-approach approach, incorporating every qualitative and quantitative information. a scientific literature evaluation comes to be executed to build up relevant studies on diabetes in early life, covering etiology, analysis, and control. additionally, a move-sectional look at become done on various patterns of pediatric diabetes patients to build up primary statistics. Questionnaires, scientific information, and interviews had been used as facts collection gear. The look aimed to apprehend the causes of diabetes in adolescents, examine the present-day traits in analysis and treatment and discover effective management strategies.
Result:
The research yielded sizeable findings in each place of investigation:
Etiology: The systematic literature compares observed a pair of things contributing to diabetes in early life. Genetic predisposition changed into an outstanding chance detail, with specific gene variants associated with improved susceptibility. additionally, environmental elements, which include nutritional behavior and lifestyle options, had been recognized as huge participants. The observation also highlighted early-lifestyles exposure's ability to ensure environmental pollutants in diabetes improvement. Evaluation The move-sectional test on pediatric diabetes sufferers helped perceive not unusual styles in the analysis and progression of the illness. The assessment found that kind 1 diabetes emerges as the maximum not unusual form in adolescence, accounting for about 80% of instances. type 2 diabetes, as soon as rare in this age institution, confirmed a concerning upward push, in standards related to weight problems and sedentary life.
Control: The studies explored numerous diabetes management techniques used in pediatric sufferers. Insulin treatment remained the cornerstone of remedy for kind 1 diabetes, however, upgrades in insulin transport structures had been found to decorate adherence and glycemic control. For kind 2 diabetes instances, lifestyle interventions, alongside eating regimen adjustments and accelerated bodily hobbies, had been critical components of control. Pharmacological treatments had been additionally tested, highlighting the efficacy and protection of certain drugs in this age organization.
Discussion
The comprehensive evaluation of diabetes in youth sheds light on the complicated interplay of genetic and environmental factors in disease improvement. The developing occurrence of type 2 diabetes in youngsters emphasized the urgent need for public health interventions to deal with early life weight problems and promote more healthy lifestyles. The study's findings additionally underlined the significance of early analysis and personalized management plans to gain higher effects in pediatric diabetes patients. The aggregate of every qualitative and quantitative statistic enriched the studies, taking into consideration more nuanced information about the multifaceted aspects of diabetes in early life. The identity of environmental pollutants as capability chance elements warrants further studies to inform preventive measures.
conclusion:
The have a take look At's findings offer valuable insights into the etiology, evaluation, and control of diabetes in early life. facts the complicated interactions between genetic predisposition and environmental influences are important for developing centered prevention strategies. Early analysis and individualized management plans preserve the important component of enhancing the lengthy-time period health consequences of pediatric diabetes patients.
The research calls for collaborative efforts amongst healthcare professionals, policymakers, and companies to deal with the developing occurrence of type 2 diabetes in youngsters via promoting healthier lifestyles and developing supportive environments. By imposing proof-based interventions, it's feasible to mitigate the load of diabetes in adolescence and beautify the amazing lifestyles of affected human beings.
Acknowledgment
The completion of this research project would not have been possible without the contributions and support of many individuals and organizations. We are deeply grateful to all those who played a role in the success of this project We would also like to thank My Mentor [. Naweed Imam Syed Prof. Department of Cell Biology at the University of Calgary and Dr. Sadaf Ahmed Psychophysiology Lab University of Karachi for their invaluable input and support throughout the research. Their insights and expertise were instrumental in shaping the direction of this project
Declaration of Interest
I at this moment declare that:
I have no pecuniary or other personal interest, direct or indirect, in any matter that raises or may raise a conflict with my duties as a manager of my office Management
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Financial support and sponsorship
No Funding was received to assist with the preparation of this manuscript
References
- Rewers M, Norris J, Kretowski A. (2009). Epidemiology of kind 1 diabetes mellitus. In: Type 1 Diabetes: mobile, Molecular & Clinical Immunology.
View at Publisher | View at Google Scholar - Rewers M, Gottlieb P. (2009). Immunotherapy for the prevention and treatment of kind 1 diabetes: human trials and a test out the destiny. Diabetes Care. 32: 1769 – 1782.
View at Publisher | View at Google Scholar - Sosenko JM, Palmer JP, Rafkin - Mervis L, Krischer JP, Cuthbertson D, et al. (2009). Incident dysglycemia and the improvement of Kind 1 diabetes amongst people within the Diabetes Prevention Trial - kind 1. Diabetes Care; 32: 1603 – 1607.
View at Publisher | View at Google Scholar - Stene LC, Barriga adequate, Hoffman M, Kean J, Klingensmith G, et al. (2006). every day but developing hemoglobin A1c stages expect development from islet autoimmunity to overt kind 1 diabetes: Diabetes Autoimmunity examines within the younger (DAISY). Pediatr Diabetes: 247 – 253.
View at Publisher | View at Google Scholar - Levy - Marchal C, Patterson CC, inexperienced A. (2001). A geographical model of the presentation at diagnosis of type 1 diabetes in children: the EURODIAB has observed it. ecu and Diabetes. Diabetologia 40-44 (Suppl three): B75 – B80.
View at Publisher | View at Google Scholar - Rewers A, Klingensmith G, Davis C, Petitti DB, Pihoker C, et al. (2008). Presence of diabetic ketoacidosis at evaluation of diabetes Mellitus in children: the search for Diabetes in teens examine. Pediatrics 121: e1258 – e1266.
View at Publisher | View at Google Scholar - Dunger DB, Sperling MA, Acerini CL, Bohn DJ, Daneman D. et al. (2004). ecu Society for Paediatric Endocrinology/Lawson Wilkins Pediatric Endocrine Society consensus announcement on diabetic ketoacidosis in children and more youthful human beings. Pediatrics. 113: e133 – e140.
View at Publisher | View at Google Scholar - Vanelli M, Chiari G, Ghizzoni L, Costi G, Giacalone T, Chiarelli F. (1999). Effectiveness of a prevention software program for diabetic ketoacidosis in kids: 8 - 365 days have a observe schools and personal practices. Diabetes Care; 22: 7 – 9.
View at Publisher | View at Google Scholar - Rewers A, Chase HP, Mackenzie T, Walravens P, Roback M. et al. (2002). Predictors of acute Headaches in kids with type 1 diabetes. JAMA. 287: 2511 – 2518.
View at Publisher | View at Google Scholar - factor JA, Jakes RW, Roy Y, Hawkins M, iciness D, et al. (2006). The UK case–manipulation seems at cerebral edema complicating diabetic ketoacidosis in kids. Diabetologia 49: 2002 – 2009.
View at Publisher | View at Google Scholar - fast PG. Diabetes education: ISPAD clinical exercising consensus hints 2006 – 2007. Pediatr Diabetes 2007; eight: 103 – 109.
View at Publisher | View at Google Scholar - Pihoker C, Forsander G, Wolfsdorf J, Klingensmith GJ. (2008). The transport of ambulatory diabetes care: systems, techniques, and results of ambulatory diabetes care. Pediatr Diabetes. nine: 609 – 620.
View at Publisher | View at Google Scholar - Bangstad HJ, Danne T, Deeb LC, Jarosz - Chobot P, Urakami T. et al. (2007). Insulin remedy: ISPAD clinical exercise consensus pointers online 2006 – 2007. Pediatr Diabetes; eight: 88 – 102.
View at Publisher | View at Google Scholar - Aslander - van VE, clever C, Waldron S. (2007). Dietary control in formative years and adolescent diabetes. Pediatr Diabetes; 8: 323 – 339.
View at Publisher | View at Google Scholar - Bantle JP, Wylie - Rosett J, Albright AL, Apovian CM, Clark NG, Franz MJ, et al. Vitamins guidelines and interventions for diabetes: a position announcement of the Yankee Diabetes affiliation. Diabetes Care 2008; 31 (Suppl 1): S61 – S78.
View at Publisher | View at Google Scholar - Robertson K, Adolfsson P, Riddell MC, Scheiner G, Hanas R. (2008). Exercising in kids and teens with diabetes. Pediatr Diabetes 9: 65 – 77.
View at Publisher | View at Google Scholar - Clarke W, Jones T, Rewers A, Dunger D, Klingensmith GJ. (2008). evaluation and management of hypoglycemia in children and young people with diabetes. Pediatr Diabetes; 9: 165 – 174.
View at Publisher | View at Google Scholar - The effect of intensive remedy of diabetes on the development and progression of long-time period headaches in insulin-structured diabetes mellitus: the Diabetes manage and complications Trial studies organization. N Engl J Med 1993; 329: 977 – 986.
View at Publisher | View at Google Scholar - Jacobson AM, Musen G, Ryan CM, Silvers N, Cleary P, et al. (2007). The long-term impact of diabetes and its treatment on cognitive features. N Engl J Med; 356: 1842 – 1852.
View at Publisher | View at Google Scholar - Chase HP. (2006). know-how Diabetes: A handbook for those who Are dwelling With Diabetes, eleventh ed. Denver, CO: kids's Diabetes basis.
View at Publisher | View at Google Scholar - Rewers M, Pihoker C, Donaghue K, Hanas R, speedy P. (2007). assessment and monitoring of glycemic control in children and youngsters with diabetes. Pediatr Diabetes; 8: 408 – 418.
View at Publisher | View at Google Scholar - Nathan DM, Cleary PA, Backlund JY, Genuth SM, Lachin JM, et al. (2005). Intensive diabetes remedy, and cardiovascular ailment in patients with type 1 diabetes. N Engl J Med. 353: 2643 – 2653.
View at Publisher | View at Google Scholar - Delamater AM. (2007). mental care of youngsters and youngsters with diabetes. Pediatr Diabetes. 8: 340 – 348.
View at Publisher | View at Google Scholar - Silverstein J, Klingensmith G, Copeland okay, Plotnick L, Kaufman F, et al. (2005). Care of children and young people with type 1 diabetes: an announcement from the Yankee Diabetes Association. Diabetes Care; 28: 186 – 212.
View at Publisher | View at Google Scholar - Maahs DM, Wadwa RP, Bishop F, Daniels SR, Rewers M. (2008). Dyslipidemia in teens with diabetes: to deal with or now not to deal with? J Pediatr; 153: 458 – 465.
View at Publisher | View at Google Scholar - McCrindle BW, Urbina EM, Dennison BA, Jacobson MS, Steinberger J. et al. (2007). Drug therapy of excessive-threat lipid abnormalities in youngsters and Children: a systematic statement from the Yankee coronary heart affiliation Atherosclerosis, high blood pressure, and obesity in young people Committee, Council of Cardiovascular Disorder within the Younger, with the Council on Cardiovascular Nursing. circulation; 115: 1948 – 1967.
View at Publisher | View at Google Scholar - Donaghue KC, Chiarelli F, Trotta D, Allgrove J, Dahl - Jorgensen okay. (2007). ISPAD clinical exercise consensus hints 2006 – 2007: Microvascular and macro vascular headaches. Pediatr Diabetes; 8: 163 –170
View at Publisher | View at Google Scholar - Rewers M, Liu E, Simmons J, Redondo MJ, Hoffenberg EJ. (2004). Celiac disease related to kind 1 diabetes mellitus. Endocrinol Metab Clin North Am; 33: 197 – 214, xi.
View at Publisher | View at Google Scholar - Barker JM. (2006). medical assessment. kind 1 diabetes-related autoimmunity: herbal history, genetic institutions, and screening. J Clin Endocrinol Metab. 91: 1210 – 1217.
View at Publisher | View at Google Scholar - Liese ad, D ' Agostino RB Jr, Hamman RF, Kilgo PD, Lawrence JM, et al. (2006). The load of diabetes mellitus amongst US youth: occurrence estimates from the look for Diabetes in teens observe. Pediatrics; 118: 1510 – 1518.
View at Publisher | View at Google Scholar
