

Case Report | DOI: https://doi.org/10.31579/2835-7957/037
De Winter Pattern: Anterior St-Elevation Myocardial Infarction Equivalent
- Amit Mandal *
Department of Cardiology C.M.C Vellore, India.Department of Cardiology C.M.C Vellore, India.
*Corresponding Author: Amit Mandal, Department of Cardiology C.M.C Vellore, India.
Citation: Amit Mandal. (2023), De Winter Pattern: Anterior St-Elevation Myocardial Infarction Equivalent, Clinical Reviews and Case Reports, 2(5); DOI:10.31579/2835-7957/037
Copyright: © 2023, Amit Mandal. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 May 2023 | Accepted: 26 September 2023 | Published: 05 October 2023
Keywords: covid-19; sars-cov-2; genome sequencing; phylogenetics
Abstract
Introduction
De winter syndrome is an unusual pattern that can occur on an electrocardiogram (ECG) [1] The de Winter pattern was first described by de Winter and colleagues in 2008 as a pattern of ECG that is associated with anterior myocardial infarction associated with left anterior descending (LAD) artery occlusion. [1] The ECG characteristics are Upsloping ST segment depression > 1mm at the J point in the precordial leads followed by Tall, prominent, symmetrical T waves in the precordial leads, other additional characteristics are slight ST-segment elevation in aVR and Absence of ST elevation in the precordial leads. [1] The de Winter pattern is seen in ~2% of acute LAD occlusions and is often under-recognised by clinicians [1]. The electrophysiological explanation of the observed ECG pattern is still unclear. Early reports of the de Winter pattern suggested that the ECG pattern is static, however there are cases reports where the de Winter pattern evolved from, or evolved to, a “classic” anterior STEMI. [2,3]. ST‐segment elevation myocardial infarction (STEMI) equivalent patterns make the diagnosis of STEMI very challenging. [1] In this paper, we discussed a case 42-year-old male with chest pain and his ECG revealing a de Winter’s pattern, showing a1to3 mm upsloping ST‐segment depression at the J point in leads V1to V6 that continues into tall, positive, and symmetrical T waves, instead of the signature ST‐segment elevation.
Case Report
A 42‐year‐old man with a history of smoking was admitted to the emergency department for recurrent chest pain for1day that had exacerbated in the previous 4 hours. The patient reported having chest pain an 8 a.m. the previous morning, radiating to the left arm and neck. Four hours before his presentation, his chest pain recurred with more intense in nature. He was admitted to the chest pain unit (CPU) with acute coronary syndrome. After admission, his myocardial enzymes were urgently examined. These showed that TnT was 34.5 pg/mL, creatine kinase MB (CKMB) was 5.5 ng/mL, potassium was 3.3 mmol/L, and he had hyperlipidaemia. The ECG showed upsloping ST‐segment depression at the J‐point with tall and symmetrical T waves from V2to V6 leads, as well as ST‐segment elevation in the aVR lead (Figure1).
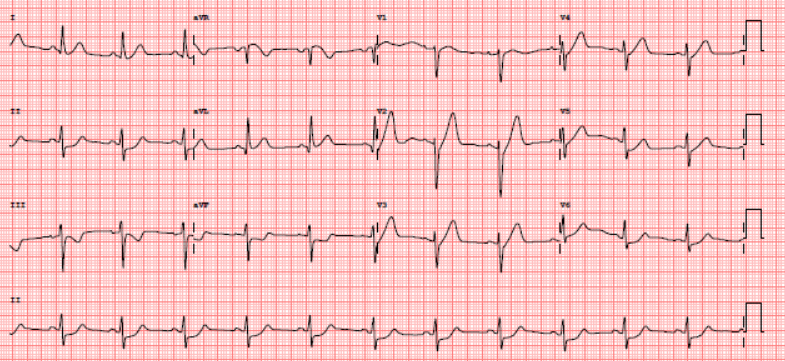
Figure 1: The electrocardiogram (ECG) shows upsloping ST‐segment depression at the J‐point with tall and symmetrical T waves from V2 to V6 leads, as well as ST‐segment elevation in the aVR lead
The ECG revealed a de Winter’s pattern, the equivalent of an anterior STEMI. After considering a diagnosis of acute myocardial infarction, he was aspirin and clopidogrel were given. The patient’s family was informed and after taking consent he was taken to the catheterization laboratory. Emergency coronary arteryangiography (CAG) revealed acute thrombotic LAD occlusion with Ostio-Proximal left anterior descending (LAD having tight lesion of 90% (Figure2).
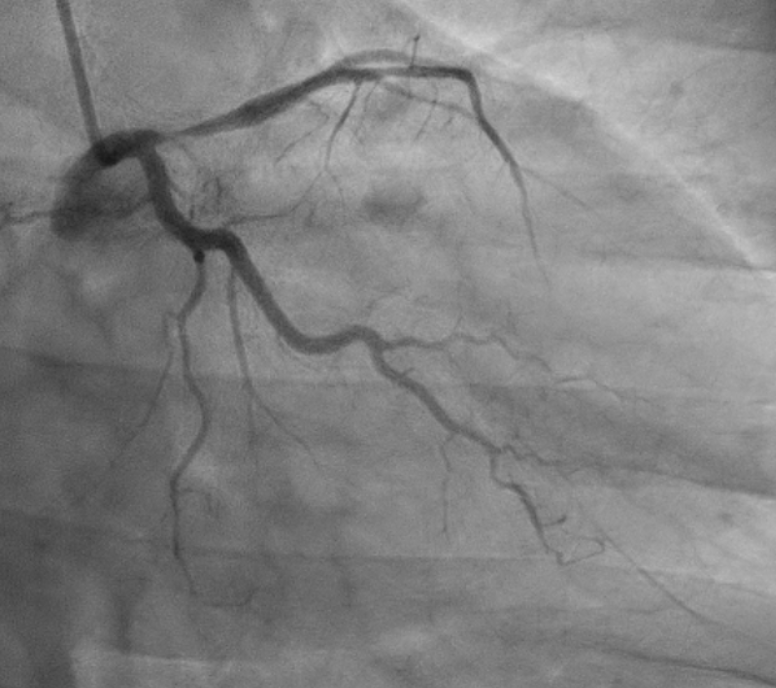

Figure 2: Coronary artery angiography (CAG) reveals acute thrombotic LAD occlusion with Ostio-Proximal left anterior descending (LAD having tight lesion of 90%
After consulting the patient’s family, a left anterior descending percutaneous coronary intervention (PCI) was performed. One drug‐eluting stent (3.5x8mm) was successfully placed in the LAD artery. A repeat angiography showed that the thrombolysis in myocardial infarction (TIMI) blood flow in the distal anterior descending artery was grade three (Figure3)
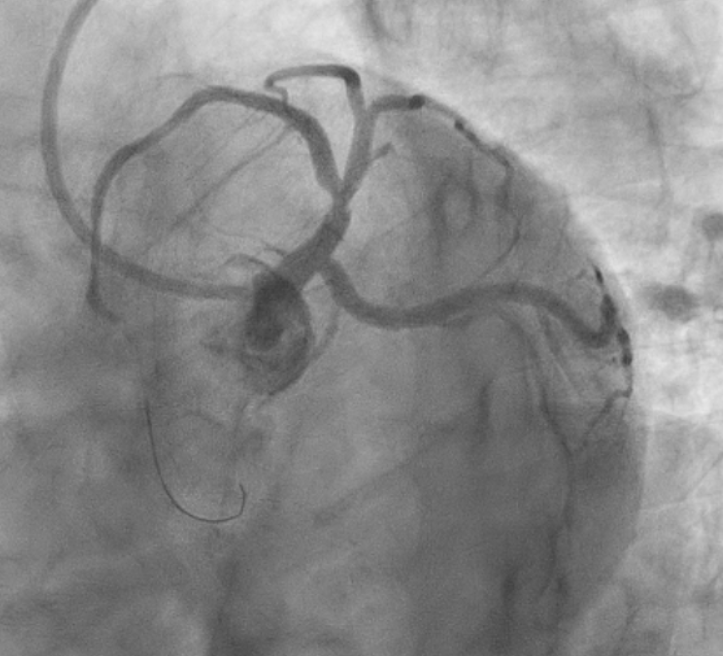
Figure 3: Repeat coronary artery angiography (CAG) after the left anterior descending percutaneous coronary intervention (PCI)
Written patient consent is present, obtained at the time of discharge. The patient was explained that his identity will not be revealed and the case information will be used for education purpose only
Discussion
characterized by a unique electrocardiogram (ECG) pattern. Epidemiological studies have revealed that de Winter syndrome is more likely to occur in male patients, who often have a younger age and frequently the comorbidity of dyslipidemia as compared with patients with STEMI [4] The clinical presentation of de Winter syndrome is mainly extensive anterior-wall myocardial infarction, which leads to left ventricular contraction dysfunction [5] The reasons for the absence of ST-segment elevation in de Winter syndrome remain unclear. However, it has been postulated the ST-segment depression and the tall peaked waves are attributed to hypoxic-driven alteration in the ATP-dependent potassium channels, which results in a delay in repolarization in the subendocardial region with change in the transmembrane action potential [6] Another theory is that a large area of transmural ischemia directs the injury current towards lead aVR and away from the precordial leads, however, this does not explain the de Winter's patter evolving into a STEMI [7] A previous study suggested that this ECG pattern was associated with the development of collateral circulation following transmural ischemia [8] Despite the consequences of this severe ECG pattern, the current guidelines by the 2017 European Society of Cardiology (ESC) and 2013 American College of Cardiology Foundation (ACCF) / American Heart Association (AHA) do not specifically address the optimal management of patients with de Winter's [9,10] . However, the ESC suggests the PCI strategy when there is a clinical concern of ongoing myocardial ischemia with STEMI criteria or atypical ECG patterns [9], hence de Winter syndrome should be considered as a high-risk STEMI and emergency revascularization is strongly recommended within the time window of intervention [8]
Since the current guidelines recommend against thrombolysis in non-STEMI and guidelines are not clear in patients with de Winter's, the usage of thrombolytic agents is still controversial. Some cases report favorable outcomes after thrombolysis [11,12]. On the other hand, one study reported two patients failing thrombolysis and one patient developing re-occlusion after a successful thrombolysis [2]
Conclusion
The de Winter's pattern indicates significant stenosis of the proximal LAD. Therefore, immediate recognition of these ECG changes is essential for referring patients to urgent reperfusion therapy and may have important prognostic implications. Guidelines are still controversial, but PCI is generally accepted and there are possible benefits of thrombolysis.
References
- De Winter RJ, Verouden NJW, Wellens HJJ, Wilde AAM. (2008). A New ECG Sign of Proximal LAD Occlusion. N Engl J Med;359(19):2071–2073.
View at Publisher | View at Google Scholar - Xu J, Wang A, Liu L, Chen Z. (2018). The de winter electrocardiogram pattern is a transient electrocardiographic phenomenon that presents at the early stage of ST‐segment elevation myocardial infarction. Clin Cardiol.;41(9):1177–1184.
View at Publisher | View at Google Scholar - Goebel M, Bledsoe J, Orford JL, Mattu A, Brady WJ. (2014). A new ST-segment elevation myocardial infarction equivalent pattern? Prominent T wave and J-point depression in the precordial leads associated with ST-segment elevation in lead aVr. Am J Emerg Med;32(3): 287.e5-287.e8.
View at Publisher | View at Google Scholar - Rokos IC, French WJ, Mattu A, Nichol G, Farkouh ME, et al. (2010). Appropriate cardiac cath lab activation: optimizing electrocardiogram interpretation and clinical decision-making for acute ST-elevation myocardial infarction. Am Heart J;160(6):995–1003, 1003.e1-1003.e8.
View at Publisher | View at Google Scholar - Martínez-Losas P, Fernández-Jiménez R. (2016).de Winter syndrome. CMAJ Can Med Assoc J J Assoc Medicale Can;188(7):528.
View at Publisher | View at Google Scholar - Tzimas G, Antiochos P, Monney P, Eeckhout E, Meier D, et al. (2019). Atypical Electrocardiographic Presentations in Need of Primary Percutaneous Coronary Intervention. Am J Cardiol;124(8):1305–1314.
View at Publisher | View at Google Scholar - Verouden NJ, Koch KT, Peters RJ, Henriques JP, Baan J. (2009). et al. Persistent precordial “hyperacute” T-waves signify proximal left anterior descending artery occlusion. Heart;95(20):1701–1706.
View at Publisher | View at Google Scholar - Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP. (2019). et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J.;40(2):87–165.
View at Publisher | View at Google Scholar - Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, et al. (2018). ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J;39(2):119–177.
View at Publisher | View at Google Scholar - O ’Gara Patrick T., Kushner FG, Ascheim DD, Casey DE, Chung MK.et al. (2013). ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction. J Am Coll Cardiol;61(4): e78–e140.
View at Publisher | View at Google Scholar - Rao MY, Wang YL, Zhang GR, Zhang Y, Liu T, et al. (2018). Thrombolytic therapy to the patients with de Winter electrocardiographic pattern, is it right? QJM;111(2):125–127.
View at Publisher | View at Google Scholar - John TJ, Pecor aro A, Weich H, Joubert L, Griffiths B. (2020). Winter’s pattern revisited: a case series. Eur Heart J - Case Rep;4(6):1–5.
View at Publisher | View at Google Scholar
