

case report | DOI: https://doi.org/10.31579/2835-7957/069
Cyst of the Thyroglossal Tract Mimicking a Laryngocele
- Loubna Taali *
- Said Anajjar
- M.Essaadi
- K.snoussi Amal Hajjij
Mohammed VI University of Health Sciences (UM6SS), Casablanca, Morocco.
*Corresponding Author: Loubna Taali, Mohammed VI University of Health Sciences (UM6SS), Casablanca, Morocco.
Citation: Loubna Taali., Said Anajjar., M.Essaadi., K.snoussi Amal Hajjij., (2024), Cyst of the Thyroglossal Tract Mimicking a Laryngocele, Clinical Reviews and Case Reports, 3(3); DOI:10.31579/2835-7957/069
Copyright: © 2024, Loubna Taali. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 14 March 2024 | Accepted: 20 March 2024 | Published: 25 March 2024
Keywords: thyroglossal tract cyst; adult; laryngocele
Abstract
The thyroglossal tract cyst (TTC) represents the most common congenital cervical mass, and it is mainly of interest to the pediatric population, with presentation in the form of a midline cervical mass. A recent lateralized or paramedian cervical mass occurring in an adult must first be eliminated as a malignant mass or laryngocele. We report the case of a 32-year-old young man, without any particular pathological history, who presented with a recent appearance of a right paramedian cervical mass adjacent to the thyroid cartilage. Preoperative CT scan revealed a cystic mass on the right, with a hemorrhagic component. Intraoperatively, the lesion was embedded in the infrahyoid muscles and it had connections with the anterior surface of the body of the hyoid bone. A Sistrunk procedure was performed. In most cases, a history and a meticulous physical examination are sufficient to make the diagnosis. The distinction between laryngocele and KTT must be made intraoperatively to avoid an inappropriate or incomplete surgical procedure. ENT surgeons must always expand the list of differential diagnoses when faced with a cervical cystic mass, in order to adapt the treatment in the event of an intraoperative surprise.
1.Introduction
cyst (TTC) has been considered the most common congenital midline anomaly in the neck [1]. The cyst usually appears as a soft, painless, slightly movable mass. Most cysts are found in the midline near the hyoid bone. However, they can be located at any location along the embryological descent pathway of thyroid tissue, thus making the diagnosis of KTT more difficult. Due to the similar manifestation of branchial cleft cysts, cystic lymphadenopathy and laryngocele , erroneous diagnoses have been made and inappropriate surgical procedures have been reported in children and adults [2,3]. KTTs are generally diagnosed before the age of 5, and 60% of lesions are diagnosed before the age of 20 . Approximately 7% of the adult population still presents this anomaly [4]. Patients with KTT typically present with a midline mass in the upper neck that moves with tongue protrusion and swallowing. The cyst is usually nontender and can reach a diameter of up to 10 cm. Although most are found in the midline, they may be less commonly located laterally, usually on the left [5]. Patients may report a recent upper respiratory infection, which may cause a sudden increase in the size of the mass [6]. The position of the KTT can be intralingual, suprahyoid, including submental, thyrohyoid or suprasternal. In approximately 60% of cases, the cyst is closely associated with the hyoid bone adjacent to the thyrohyoid membrane [5].
Case presentation
A 3 2-year-old male presented with a right neck mass noted 2 months previously. He had no history of trauma or oncology or toxic risk factors, such as tobacco, alcohol or exposure to radiation. On the other hand, he complained of slight dyspnea upon exertion, with dysphonia, with a context of vocal straining. Physical examination revealed a 4 cm right paramedian cervical mass (figure 1),

Figure 1: L’examen physique a objectivé une masse cervicale paramédiane droite de 4 cm
slightly tender, soft, mobile and compressible, adjacent to the thyroid cartilage, which does not move with swallowing. The lymph node areas were free. And the rest of the ENT clinical examination was normal.
A flexible nasofibroscopy showed a normal-appearing larynx, with normal mobility of the vocal cords. (Figure2)

Figure 2 : Aspect et mobilité normales du larynx à l’endoscopie
Ultrasound showed an oval, thick-contoured, thick-walled cystic formation measuring 36x26cm. (figure 3).
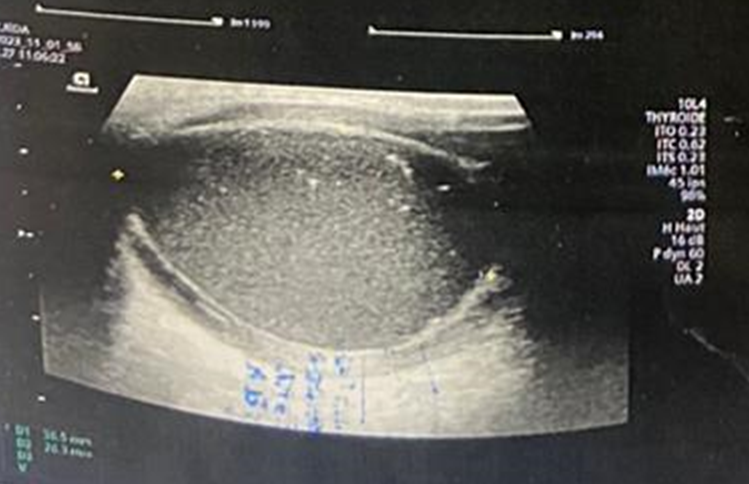
Figure 3: échographie cervicale montrant une formation ovalaire, kystique à contours épais, à paroi épaisses, mesurant 36x26cm.
A cervical CT scan confirmed the cystic nature of the mass, which was right paramedian, coming into contact with the thyroid cartilage and the thyrohyoid membrane (figure 4) with hematic rearrangement in its lower part.
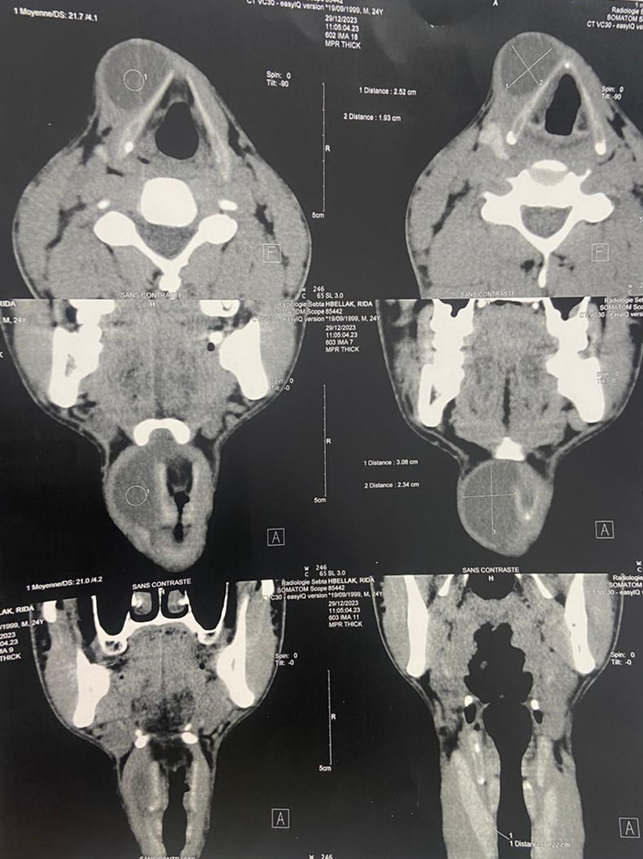
Figure 4 : scanner cervical en coupes axiales et coronales montrant une masse kystique de paramédiane droite, arrivant au contact du cartilage thyroïde et la membrane thyro-hyoidienne , avec remaniement hématique dans sa partie inférieure.
This mass pushed the larynx slightly to the left. The diagnosis of laryngocele was raised. Intraoperatively, the cyst was encountered below the right subhyoid muscles, with intimate contact with the thyroid cartilage and the thyrohyoid membrane ,and connections with the body of the hyoid bone. (Figure 5)
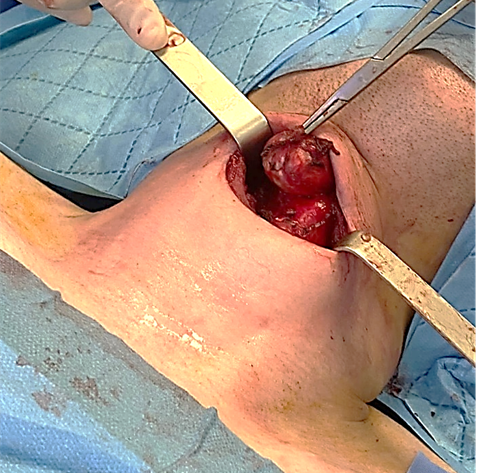
Figure 5A : Vue per opératoire du kyste : le kyste a été rencontré au-dessous des muscles sous hyoidiens droits, avec contact intime avec le cartilage thyroidien et la membrane thyro- hyoïdienne
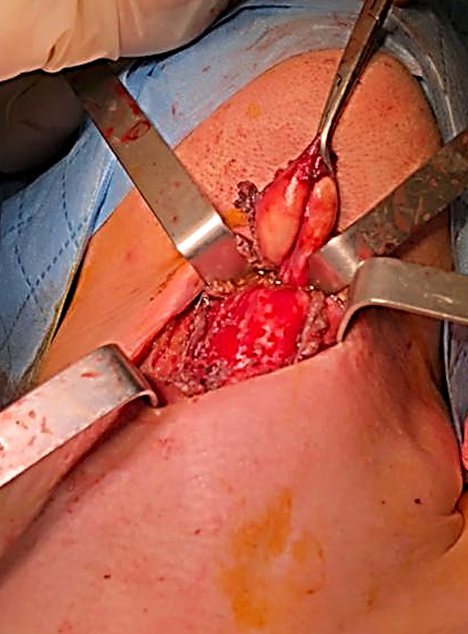
Figure 5 B :Vue per opératoire du kyste :notez les connections avec le corps de l’os hyoïde en haut
An exploratory cervicotomy was performed. Given the intraoperative appearance which favors a KTT, and the confirmation of the normal position of the thyroid gland on imaging, a complete Sistrunk procedure was performed. The post-operative aftermath was simple. study of the mass revealed a benign squamous cyst with marked inflammatory changes, consistent with KTT.
Case presentation
A 3 2-year-old male presented with a right neck mass noted 2 months previously. He had no history of trauma or oncology or toxic risk factors, such as tobacco, alcohol or exposure to radiation. On the other hand, he complained of slight dyspnea upon exertion, with dysphonia, with a context of vocal straining. Physical examination revealed a 4 cm right paramedian cervical mass (figure 1),

Figure 1: L’examen physique a objectivé une masse cervicale paramédiane droite de 4 cm
slightly tender, soft, mobile and compressible, adjacent to the thyroid cartilage, which does not move with swallowing. The lymph node areas were free. And the rest of the ENT clinical examination was normal.
A flexible nasofibroscopy showed a normal-appearing larynx, with normal mobility of the vocal cords. (Figure2)

Figure 2 : Aspect et mobilité normales du larynx à l’endoscopie
Ultrasound showed an oval, thick-contoured, thick-walled cystic formation measuring 36x26cm. (figure 3).
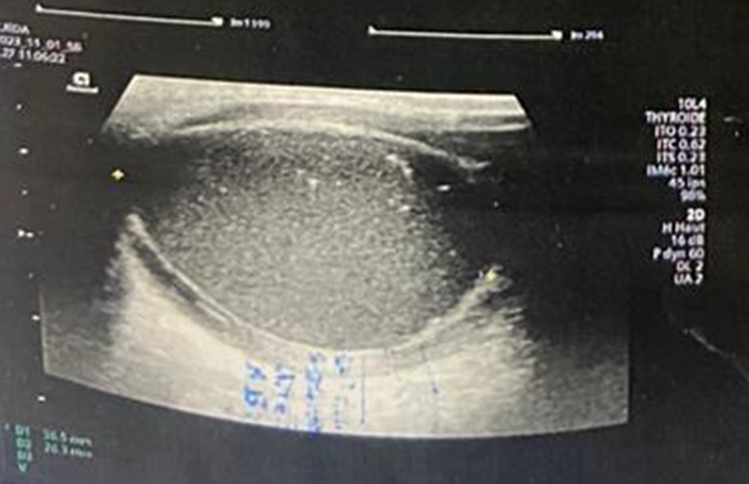
Figure 3: échographie cervicale montrant une formation ovalaire, kystique à contours épais, à paroi épaisses, mesurant 36x26cm.
A cervical CT scan confirmed the cystic nature of the mass, which was right paramedian, coming into contact with the thyroid cartilage and the thyrohyoid membrane (figure 4) with hematic rearrangement in its lower part.
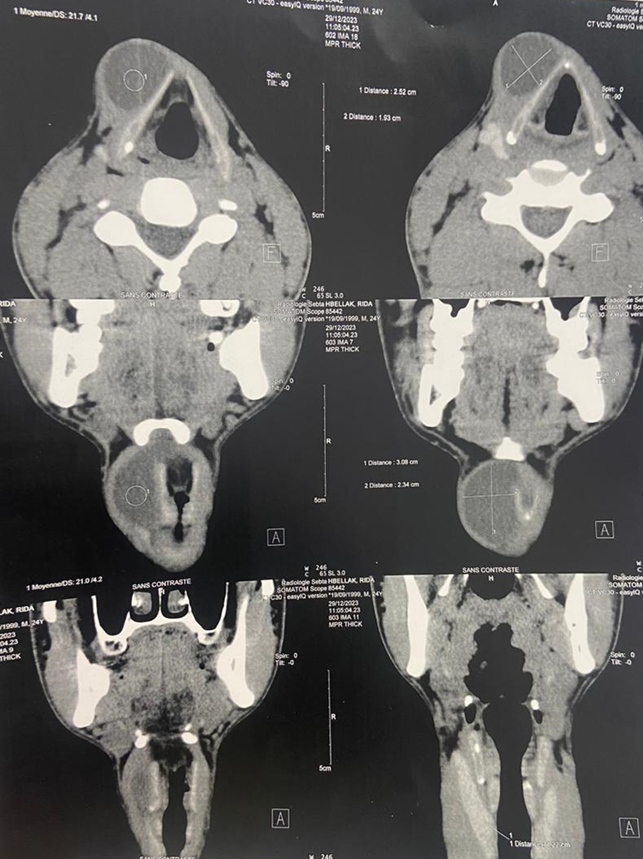
Figure 4 : scanner cervical en coupes axiales et coronales montrant une masse kystique de paramédiane droite, arrivant au contact du cartilage thyroïde et la membrane thyro-hyoidienne , avec remaniement hématique dans sa partie inférieure.
This mass pushed the larynx slightly to the left. The diagnosis of laryngocele was raised. Intraoperatively, the cyst was encountered below the right subhyoid muscles, with intimate contact with the thyroid cartilage and the thyrohyoid membrane ,and connections with the body of the hyoid bone. (Figure 5)
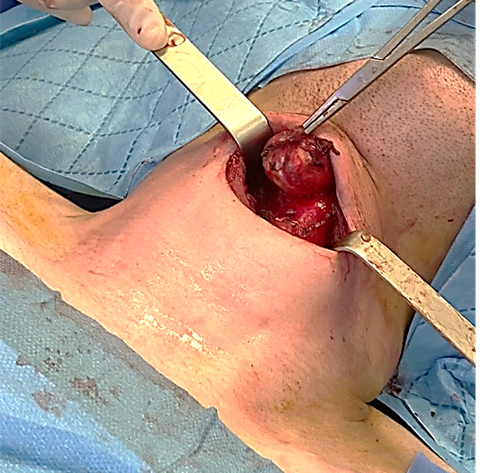
Figure 5A : Vue per opératoire du kyste : le kyste a été rencontré au-dessous des muscles sous hyoidiens droits, avec contact intime avec le cartilage thyroidien et la membrane thyro- hyoïdienne
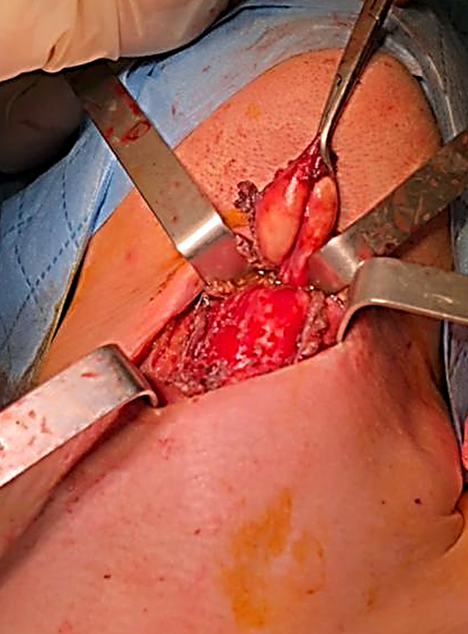
Figure 5 B :Vue per opératoire du kyste :notez les connections avec le corps de l’os hyoïde en haut
An exploratory cervicotomy was performed. Given the intraoperative appearance which favors a KTT, and the confirmation of the normal position of the thyroid gland on imaging, a complete Sistrunk procedure was performed. The post-operative aftermath was simple. study of the mass revealed a benign squamous cyst with marked inflammatory changes, consistent with KTT.
Case presentation
A 3 2-year-old male presented with a right neck mass noted 2 months previously. He had no history of trauma or oncology or toxic risk factors, such as tobacco, alcohol or exposure to radiation. On the other hand, he complained of slight dyspnea upon exertion, with dysphonia, with a context of vocal straining. Physical examination revealed a 4 cm right paramedian cervical mass (figure 1),

Figure 1: L’examen physique a objectivé une masse cervicale paramédiane droite de 4 cm
slightly tender, soft, mobile and compressible, adjacent to the thyroid cartilage, which does not move with swallowing. The lymph node areas were free. And the rest of the ENT clinical examination was normal.
A flexible nasofibroscopy showed a normal-appearing larynx, with normal mobility of the vocal cords. (Figure2)

Figure 2 : Aspect et mobilité normales du larynx à l’endoscopie
Ultrasound showed an oval, thick-contoured, thick-walled cystic formation measuring 36x26cm. (figure 3).
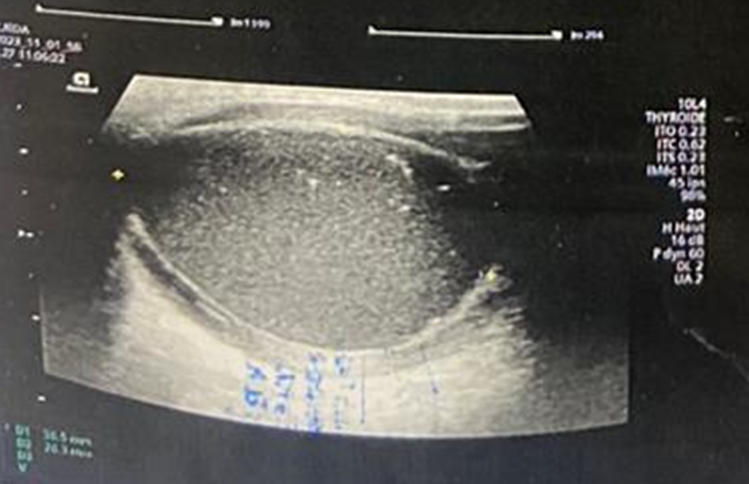
Figure 3: échographie cervicale montrant une formation ovalaire, kystique à contours épais, à paroi épaisses, mesurant 36x26cm.
A cervical CT scan confirmed the cystic nature of the mass, which was right paramedian, coming into contact with the thyroid cartilage and the thyrohyoid membrane (figure 4) with hematic rearrangement in its lower part.
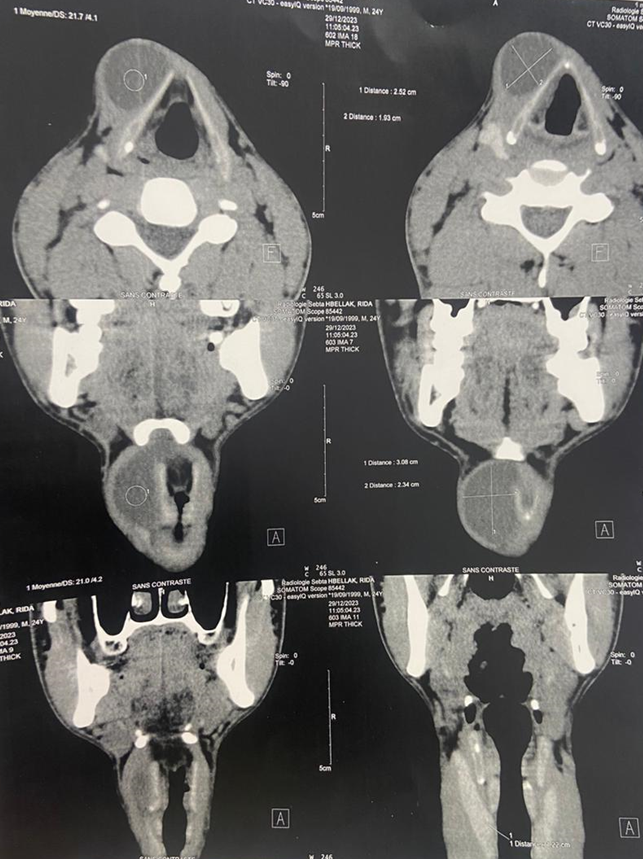
Figure 4 : scanner cervical en coupes axiales et coronales montrant une masse kystique de paramédiane droite, arrivant au contact du cartilage thyroïde et la membrane thyro-hyoidienne , avec remaniement hématique dans sa partie inférieure.
This mass pushed the larynx slightly to the left. The diagnosis of laryngocele was raised. Intraoperatively, the cyst was encountered below the right subhyoid muscles, with intimate contact with the thyroid cartilage and the thyrohyoid membrane ,and connections with the body of the hyoid bone. (Figure 5)
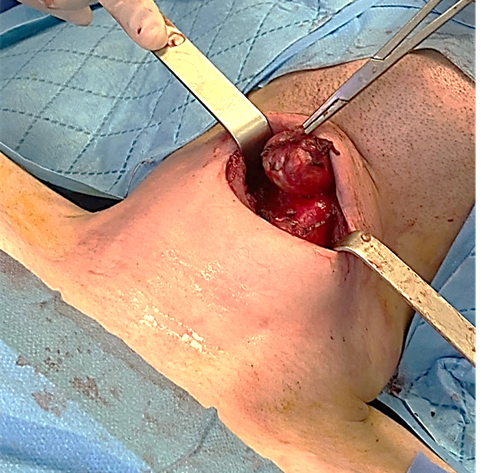
Figure 5A : Vue per opératoire du kyste : le kyste a été rencontré au-dessous des muscles sous hyoidiens droits, avec contact intime avec le cartilage thyroidien et la membrane thyro- hyoïdienne
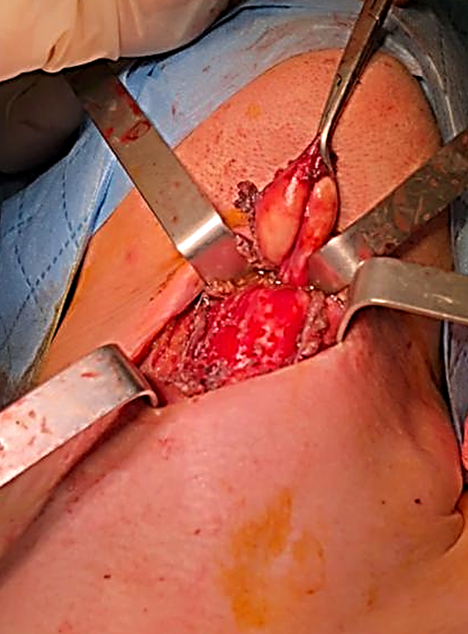
Figure 5 B :Vue per opératoire du kyste :notez les connections avec le corps de l’os hyoïde en haut
An exploratory cervicotomy was performed. Given the intraoperative appearance which favors a KTT, and the confirmation of the normal position of the thyroid gland on imaging, a complete Sistrunk procedure was performed. The post-operative aftermath was simple. study of the mass revealed a benign squamous cyst with marked inflammatory changes, consistent with KTT.
Discussion
Adult KTTs are distinguished from the pediatric form by their size, so they are more symptomatic. Adults are more likely than children to present with
symptoms other than a mass or infection, namely pain, sore throat, dysphagia, hoarseness, and fistulization of the mass [7]. The differential diagnosis of a KTT mainly includes dermoid cysts, sebaceous cysts, branchial cleft cysts, thyroid nodules, lymphadenopathy and lipomas, and laryngoceles. Diagnosis of KTT relies largely on a thorough history and examination of the head and neck. Ultrasound, CT, and MRI are all good tools for the positive and differential diagnosis of thyroglossal duct cysts, but sometimes confirmation remains intraoperative [8]. Cysts of the thyroglossal tract are sometimes of surprising location, varying in height along the laryngeal axis. Some cases can mimic a laryngeal cyst, with a picture of dyspnea in particular due to compression of the cricothyroid membrane, leading to a narrowing of the subglottic tract in its anterior part. Clinically, the absence of mobility of the mass during swallowing and tongue protraction should not eliminate the diagnosis of KTT. Our case illustrates the importance of broadening the list of differential diagnoses and detailing radiological examinations in order to ensure appropriate management, despite clinical characteristics that suggest another diagnosis. The diagnosis is sometimes intraoperative. Although we ultimately retained the diagnosis of KTT, certain preoperative features of this case indicated a laryngocele. First, the lesion was paramedian. Generally, lateralization is more suggestive of an external laryngocele than of a KTT. Secondly, male gender and the appearance of the mass in adulthood corresponds better to that of laryngocele , in fact 60% of KTT are diagnosed before the age of 20 [4]. ; In an adult presenting with a benign lateral cervical mass, the diagnostic hypothesis of laryngocele is more probable than thyroglossal duct cysts, especially in the presence of a risk factor such as vocal straining, or the notion of playing games. wind instruments and the glass blower. Intraoperatively, the origin of the lesion in our case was judged more compatible with a KTT than with a laryngocele, and the operative management was therefore modified to ensure complete excision. Surgical procedures for laryngocele and KTT differ. Treatment of a laryngocele involves resecting the cyst itself, which may include part of the laryngeal mucosa [9]. In contrast, a KTT is treated with a Sistrunk procedure which removes the cyst and its tract, as well as the center of the hyoid bone and leaves the mucosa of the larynx and pharynx intact [10]. If a KTT is confused with a laryngocele, the hyoid bone would remain in place, leading to recurrence [11,12]. Renee Booth et al reported a case similar to ours, it involves a KTT mimicking a laryngocele. The definitive diagnosis was established intraoperatively, the lesion was directed towards the hyoid bone; a Sistrunk procedure was performed [12]. Yamada et al [13] and Wakasa et all [14] both reported cases of adults with KTT presenting as asymptomatic lateral neck masses; mimicking a branchial cleft cyst, the two surgeons did not perform the Sistrunk procedure. These cases illustrate the interest in including KTT in the list of diagnoses to be considered for asymptomatic lateral cervical masses in adults. Furthermore, the occasional presence of micro carcinoma in these cysts can lead to metastases if the diagnosis is not identified and treated [15].
Conclusion
thyroglossal tract cysts (TTCs) are most commonly present in the pediatric population as midline masses, they can also present in adults and may be lateralized. Their surgical management requires a Sistrunk procedure, that is to say the removal of the center of the hyoid bone. For this reason, medial or paramedian cystic lesions should be subject to further intraoperative investigation when KTT is considered as a differential diagnosis.
References
- Ryu J, Igawa T, Mohole J, Coward M. (2023). Congenital Neck Masses. Neoreviews. ;24(10) : e642-e649.
View at Publisher | View at Google Scholar - Radioisotope Scanning of the Thyroid Gland Prior to Thyroglossal Duct Cyst Excision .David E. Tunkel, MD; Edgar E. Domenech, MD Arch Otolaryngol Head Neck Surg. 1998;124(5):597-599.
View at Publisher | View at Google Scholar - Thyroglossal Duct Remnants Preoperative Evaluation and Management Diana Radkowski, MD; James Arnold, MD; Gerald B. Healy, MD; et alTrevor McGill, MD; S. T. Treves, MD; Harriet Paltiel, MD; Ellen M. Friedman, MD. Arch Otolaryngol Head Neck Surg. 1991;117(12):1378-1381.
View at Publisher | View at Google Scholar - Gorlin R.J., Goldman H.M., et al. (1972). Hurt W. : La pathologie buccale de Thoma. J Parodontol, n° 43, p. 575 à 577
View at Publisher | View at Google Scholar - Shah R, Gow K, Sobol SE. (2007). Outcome of thyroglossal duct cyst excision is independent of presenting age or symptomatology. Int J Pediatr Otorhinolaryngol. ;71(11):1731-1735.
View at Publisher | View at Google Scholar - Noyek AM, Friedberg J. (1981). Thyroglossal duct and ectopic thyroid disorders. Otolaryngol Clin North Am. ;14(1):187-201.
View at Publisher | View at Google Scholar - Brousseau VJ, Solares CA, Xu M, Krakovitz P, Koltai PJ. (2003). Thyroglossal duct cysts: presentation and management in children versus adults. Int J Pediatr Otorhinolaryngol. 67(12):1285-1290.
View at Publisher | View at Google Scholar - Tokarz E, Gupta P, McGrath J, Szymanowski AR, Behar J, Behar P. (2021). Proposed ultrasound algorithm to differentiate thyroglossal duct and dermoid cysts. Int J Pediatr Otorhinolaryngol.142:110624.
View at Publisher | View at Google Scholar - Dursun G, Ozgursoy OB, Beton S, Batikhan H. (2007). Current diagnosis and treatment of laryngocele in adults. Otolaryngol Head Neck Surg.136(2):211-215.
View at Publisher | View at Google Scholar - Gioacchini FM, Alicandri-Ciufelli M, Kaleci S, Magliulo G, Presutti L, Re M. (2015). Clinical presentation and treatment outcomes of thyroglossal duct cysts: a systematic review. Int J Oral Maxillofac Surg.44(1):119-126.
View at Publisher | View at Google Scholar - Geller KA, Cohen D, Koempel JA. (2014). Thyroglossal duct cyst and sinuses: a 20-year Los Angeles experience and lessons learned. Int J Pediatr Otorhinolaryngol;78(2):264-267.
View at Publisher | View at Google Scholar - Booth R, Tilak AM, Mukherjee S, Daniero J. (2019). Thyroglossal duct cyst masquerading as a laryngocele. BMJ Case Rep. 12(3):e228319.
View at Publisher | View at Google Scholar - Yamada S, Noguchi H, Nabeshima A, Tasaki T, Kitada S. et al. (2013). Papillary carcinoma arising in thyroglossal duct cyst in the lateral neck. Pathol Res Pract. 209(10):674-678
View at Publisher | View at Google Scholar - Wakasa Y, Oishi S, Nara M, Nozaki T, Yoshihara S. et al. (2017). Papillary Carcinoma Arising in Thyroglossal Duct Cyst in the Right Lateral Neck. Gan To Kagaku Ryoho. 44(12):1152-1154.
View at Publisher | View at Google Scholar - Gómez- Álvarez LR, Treviño -Lozano MA, de la O- Escamilla ME, Vergara -Miranda H, Anda LAM. (2022). Papillary thyroid carcinoma from a thyroglossal cyst : case series . J Surg Case Rep. (2): rjab613
View at Publisher | View at Google Scholar
