

Short communication | DOI: https://doi.org/10.31579/2835-7957/057
Calculation of average waiting time from diagnosis till surgical intervention for minor and day case general surgical procedures
- Aliya Ishaq *
- Muhammad Jamshaid Husain Khan
- Almaha Khaled Almahri
- Mizna Mustafa
- , Neeha Tahir
- Suhana Riyaz
- Asma Tariq
- Khadija Abdullah Alhebsi
- Reem Abdallah
- Esaaf Hasan Ghazi
- Arfan Al Awa
- Zaid Abdelaziz
1 Department of Thyroid and Breast Surgery, Weifang Hospital of Traditional Chinese Medicine, China.
2 Medical imaging department, Weifang Hospital of Traditional Chinese Medicine, China.
*Corresponding Author: Aliya Ishaq, Department of General Surgery, Dubai Hospital.
Citation: Aliya Ishaq., Husain Khan MJ., Almaha K. Almahri., Mizna Mustafa., Neeha Tahir, et al, (2024), Calculation of average waiting time from diagnosis till surgical intervention for minor and day case general surgical procedures, Clinical Reviews and Case Reports, 3(2); DOI:10.31579/2835-7957/057
Copyright: © 2024, Aliya Ishaq. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 December 2023 | Accepted: 16 January 2024 | Published: 30 January 2024
Keywords: surgical intervention; surgical procedures; general surgery
Abstract
Waiting period for elective surgery is a major health concern for major commonwealth countries. Waiting periods for elective healthcare services have been a policy concern in most developed countries' health systems. Many nations have made efforts to reduce surgical wait times despite limited resources. These efforts encompass streamlining the process from consultation to the actual procedure. They can provide an opportunity for policymakers to make necessary adjustments to enhance the appropriateness, responsiveness, and efficiency of healthcare delivery
Introduction
Waiting period for elective surgery is a major health concern for major commonwealth countries. Waiting periods for elective healthcare services have been a policy concern in most developed countries' health systems. Many nations have made efforts to reduce surgical wait times despite limited resources. These efforts encompass streamlining the process from consultation to the actual procedure. They can provide an opportunity for policymakers to make necessary adjustments to enhance the appropriateness, responsiveness, and efficiency of healthcare delivery [1]. Ultimately, these adjustments aim to create health systems that are more focused on meeting the individual's healthcare needs effectively. Various Initiatives are introduced to reduce the waiting period with varying success. Ensuring timely access to elective surgical care in publicly funded healthcare systems remains a significant challenge. The analysis on time trends serves to identify countries that have successfully and significantly reduced waiting times. ‘Surgical wait time’ refers to the time from the decision to operate to the operation itself, however, this definition only accounts for a fraction of the actual wait time experienced by the patient [2] A more realistic model might begin at a patient’s first visit to a health care provider followed by their referral to first clinic visit, diagnosis and ultimately only the last component will be the decision to perform surgical operation. As strategies are implemented to decrease wait times, it will become increasingly important to monitor the entire wait time from referral to operation because the time prior to the decision to operate represents a significant portion of the wait time and when current wait times are compared to those in the future, it will be useful to see which component of the wait is increasing or decreasing and how this is related to the wait time strategies implemented at the provincial and institutional level[3]. Waiting lists may have positive benefits. In the face of scarce resources, rationing by waiting may be considered preferable to rationing by price. Time spent waiting might allow recovery to occur without surgical intervention. Waiting lists permit efficient use of resources and enable scheduling to ensure a balanced case load. On the negative side, waiting for treatment which has already been judged clinically necessary may be considered unacceptable, conditions may deteriorate during the wait and waiting may cause considerable pain and distress. Average waiting time from day of surgical decision till date of surgery is reported between 30-57 days in different series. Delays are reported by 16.8% of patients; most common delays are operating room cancellations/time constraints, patients requiring further optimization and delays in referral (4.7%, 3.4% and 3.1%, respectively) [1]. We did an audit in our department to calculate the waiting time from diagnosis till surgical intervention for minor and day case general surgical procedures form from jan 2022 till June 14 2023 .
Methodology:
Data Collection method: Retrospective from the electronic medical record system.
Population & time period; All patient who had minor and day case general surgical procedures between jan 2022 till June 14 2023.
Exclusion Criteria: Emergency cases.
Project Sample Size: 80-100
Sample selection: Convenient sampling.
Resultrs ;
Total 286 cases were operated from jan 2022 till June 14 2023.
List of cases operated is as follows;
• Hernias, inguinal and umbilical. •
. Mastectomies, subcutaneous for gynecomastia •
. Lipomas.
•Hemorrhoids.
• Fistula in ano .
• Fissure in ano .
• Pilonidal sinus .
• breast lumpectomies.
• Excision of accessory breast.
• Excision breast biopsies.
• Secondary closures.
• Wound debridement.
• Toe nails
• Abscesses.
• Nipple surgeries.
• Skin tag.
• Lymph node biopsies
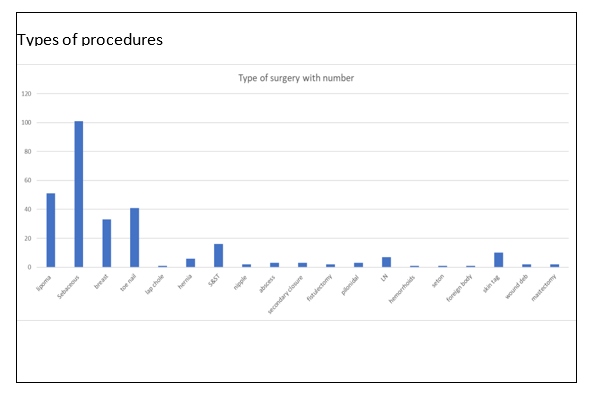
Different procedures performed are represented in chart 1 ;
Chart 1 :
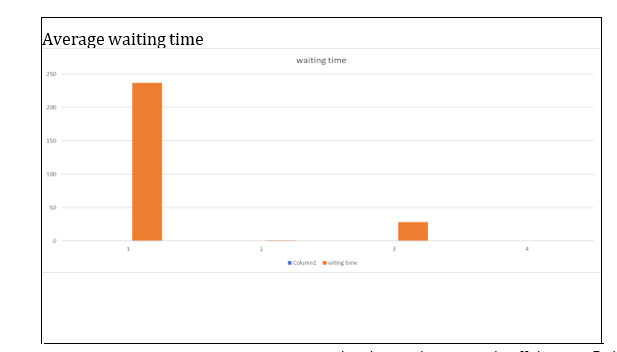
Average waiting time for all procedures is presented in chart 2 ;
Chart 2:
The average waiting time for all procedures was 28.6 days, which is lower than the reported range of 30-57 days in the literature. The largest waiting time of 237 days for two patients was attributed to pregnancy and bronchitis. While other delays occurred due to personal reasons, delays in imaging appointments, and staff shortages. Patient selection criteria were established for day case surgeries, and future plans include expanding the
range of procedures performed in the day care unit to include laparoscopic cholecystectomy, lumpectomy, sleeve gastrectomy, and other hernia types. With an average waiting time of only 28.6 days, our facility has
consistently outperformed the reported range of 30-57 days found in the literature, indicating an efficient and streamlined process for patients seeking surgical procedures. We had two delayed procedures due to one of the patients becoming pregnant and the surgery was done in the second trimester. Another patient had bronchitis and that delayed the surgery until he was vitally stable.
Discussion:
although surgery waiting time cannot be eliminated it can be improved. After analyzing the waiting time for a total of 286 procedures, the average time was lower than the ranges reported in literature. This shows the efficacy of the efforts put in to reduce the waiting time and if continued there can be significant changes in the healthcare system. The different strategies mentioned have proved their positive impact in improving the wait time and with the cooperation of multiple sectors in healthcare, waiting time can be drastically improved for the patient’s benefit as well as the healthcare systems. Numerous strategies were found and have been shown positive evidence of their effectiveness in reducing the wait time[1],some of which include encompassing expanded roles for non-physicians, process improvement methodologies, publicly funded surgeries in private facilities, same-day surgery and discharge, standardized treatment pathways, streamlined pre-admission processes, targeted funding, centralized elective surgeries, centralized surgical scheduling, efficient use of operating rooms, family doctors-led surgeries, fast-track programs, patient choice, mobile surgical clinics, organization incentives, appointment reminders, cancellation lists, flex days, and innovative surgical approaches have been implemented to reduce wait times for elective surgeries, each showcasing varying degrees of success and impacts[2]. These approaches have collectively addressed the challenge of lengthy wait times for elective procedures in healthcare systems, ultimately streamlining processes and improving patient access to timely care[3] . Reducing waiting times for elective surgeries is a complex challenge that demands a holistic approach, underscoring the critical importance of assembling a multidisciplinary team encompassing various specialties and involving all sectors of healthcare. Collaboration among professionals from different fields, including surgeons, nurses, anesthesiologists, and administrative staff, is vital in optimizing the surgical process. This collaborative effort streamlines pre-operative assessments, surgery scheduling, and post-operative care, ultimately resulting in shorter waiting times for patients [1]. Moreover, it allows for the efficient allocation of resources and expertise, enabling healthcare systems to meet the growing demand for elective surgeries and enhance the overall quality of patient care [2].
Conclusion:
Waiting time is an increasingly popular measure of health care delivery and is one of the key performance indicator for a health care system. Currently, ‘surgical wait time’ often refers to the time from the decision to operate to the operation itself, however, this definition only accounts for a fraction of the actual wait time experienced by the patient[i]. Delaying treatment has unfavorable effects on patient outcome. Our Average waiting time for day case surgeries is acceptable as per international standards for general surgical day case procedures . Establishment of one step clinic with anesthesia and other teams to expedite the evaluation and optimization of patients for day case can further attempt to reduce waiting time and patient anxiety as is Involvement of fast tract services with radiology and other specialties when needed to expedite the process of preparation of patient for safe day case surgery. Day case units should have senior experienced staff available for patient admission and assessment before discharge.
More complex cases can be included as day cases in future provided above requirements are met.
References
- L. Siciliani et al. (2014). Measuring and comparing health care waiting times in OECD countries; Health Policy 118. 292–303.
View at Publisher | View at Google Scholar - Cole E, Hopman W, Kawakami J. (2011). High resolution analysis of wait times and factors affecting surgical expediency. Can Urol Assoc J.5(1):13-17.
View at Publisher | View at Google Scholar - Fernanda N. I. Nagase et al. (2022). Reducing the wait for surgical consultation—what works and what doesn’t? —a review of selected countries in North America, Europe and Australasi; d. J Hosp Manag Health Policy;6:2
View at Publisher | View at Google Scholar - Eric Cole, Wilma Hopman, MA; † Jun Kawakami. (2011). High resolution analysis of wait times and factors affecting surgical expediency; : Can Urol Assoc.5(1):13-17.
View at Publisher | View at Google Scholar - Stafinski, Tania, et al. (2022). “Reducing Wait Times to Surgery-an International Review.” Journal of Hospital Management and Health Policy, AME Publishing Company, 25 Sept.
View at Publisher | View at Google Scholar - Kreindler SA. (2010). Policy strategies to reduce waits for elective care: a synthesis of international evidence. Br Med Bull; 95:7-32.
View at Publisher | View at Google Scholar - Downey M. (2014).Transformative cardiac care model streamlines procedures and reduces wait times. Ottawa (ON), Canada: Canadian Foundation for Healthcare Improvement.
View at Publisher | View at Google Scholar - Ghai S, Lee SY, Bret PM, et al. (2015). Thyroid Biopsy Specialists: A Quality Initiative to Reduce Wait Times and Improve Adequacy Rates. Radiology. 276:894-899.
View at Publisher | View at Google Scholar - Scottish Government. (2017). The Modern Outpatient: A Collaborative Approach 2017-2020. Edinburgh, Scotland: Scottish Government.
View at Publisher | View at Google Scholar - Kawakami J, Hopman WM, Smith-Tyron R, et al. (2008). Measurement of surgical wait times in a universal health care system. Can Urol Assoc J. 2:597-603
View at Publisher | View at Google Scholar
