

Research Article | DOI: https://doi.org/10.31579/2835-7957/007
Assessing Empathy Levels among Medical Students at Sultan Qaboos University in Sultanate of Oman
- Hamed Al Sinawi *
- Noor Mohammed Ahmed Alkaabi
- Anfal Saif Ali Al-Subhi
- Abdulrahman Al-Mirza
Sultan Qaboos University College of Medicine, Sultanate of Oman-Muscat, Al-khoudh, Oman.
*Corresponding Author: Hamed Al Sinawi, Senior consultant psychiatrist, Sultan Qaboos, University Hospital, Sultanate of Oman-Muscat, Al-khoudh, Oman.
Citation: Hamed Al Sinawi, Noor Mohammed Ahmed Alkaabi, Anfal Saif Ali Al-Subhi, Abdulrahman Al-Mirza (2022) Assessing Empathy Levels among Medical Students at Sultan Qaboos University in Sultanate of Oman. Clinical Reviews and Case Reports.1(2); DOI:10.31579/2835-7957/007
Copyright: © 2022, Hamed Al Sinawi, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 December 2022 | Accepted: 13 December 2022 | Published: 26 December 2022
Keywords: empathy, interpersonal reactivity index, pre-clinical, clinical, medical students
Abstract
Introduction
The patient-doctor relationship has a significant contribution to the outcome of health care services. One of the most important doctor’s qualities is empathy. There are plenty of definitions for empathy, but broadly, it is considered an essential effective mode of understanding [1]. There are two primary components of empathy, cognitive and affective. Cognitive empathy is the ability to understand the feeling of others [2] and take their perspective [3]. In contrast, affective empathy is an emotional reflection of cognitive empathy [4]. Neurological studies evidence that the brain pain areas are stimulated while watching someone else’s pain [5][6].
Considering the outcomes and consequences of empathy, it has a very high value in a doctor’s personality as it eases the communication process between the doctor and his patients; hence, it increases the levels of trust [7]. Due to the solid doctor-patient relationship, patients tend to open up themselves and tell their symptoms and history accurately, eventually resulting in a more accurate diagnosis [8]. Furthermore, it has been found that empathy itself plays a significant role in improving the therapy outcome as it relaxes the patients, relieves their anxiety [9], and facilitates adherence to therapy [8]. As previous studies stated, plenty of factors contribute to the level of empathy a doctor might have. Those factors are; gender, the number of study years, community, parents' marital status, future specialization, and other factors.
Clinical empathy is an essential component of professionalism in medical practice and is very necessary for the future of health. Apart from age, gender, and culture, several factors can improve and maintain clinical empathy in medical students, such as undergraduate courses about the context and timing of clinical experience and communication skills training.
Materials and Methods
Study design and data collection
This is a cross-sectional study conducted among 500 medical students at SQU, from 1st to last year, from both genders during the academic year 2019-2020. We randomly selected a group of medical students from the medicine and health science college at SQU to participate in a pilot study by completing the Interpersonal Reactivity Index (IRI). IRI survey consisted of 28 questions (9 negatively worded) that were subdivided into four subscales which are, Perspective Taking (PT), Empathic Concern (EC), Personal Distress (PD), and Fantasy Sale (FS) as attached in index 1. Then we received their feedback on the clarity of the questions and any suggested modifications. Ethical approval was obtained from the Medical Research Committee at SQU in October 2019 (#1994). Data collection started using IRI and specifically designed a data collection sheet about the student's age, gender, year of study, and if the students live alone or with their families.
Data analysis
After conducting the survey, data was created and analyzed using the Statistical Package for Social Sciences (SPSS) (23rd version). The categorized variables were displayed in the form of percentages in frequency tables and bar charts. For comparing continuous variables (mean) of two categorized variables, the Mann-Whitney U test was used. A P-value of <0>
Results
Demographic characteristics
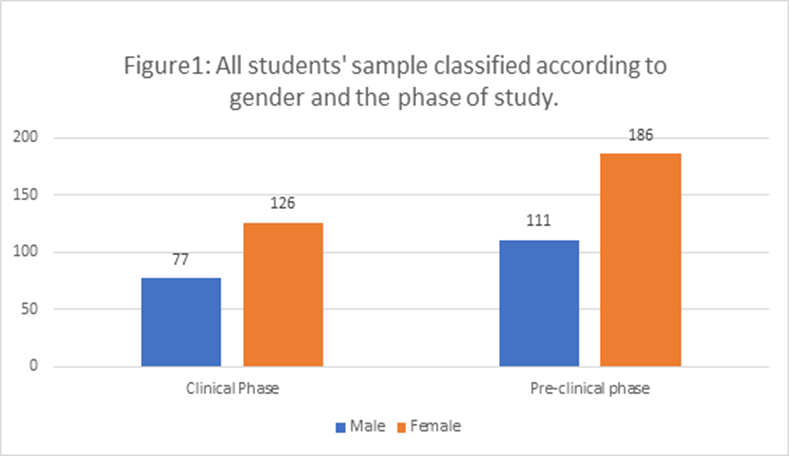
The questionnaire was completed by 500 medical students who were accepted to participate in this study. There were 188 (37.6Percentage) males and 312 (62.4Percentage) females. Regarding the phases of the study, there were 297 (59.4Percentage) students in the pre-clinical phase and 203 (40.6Percentage) students in the clinical phase (Figure1).
Level of empathy among medical students at SQU.
The IRI was subcategorized into its four sub-scales, EC, PT, PD, and FS. Then Mean±SD was obtained for the sub-scales as shown in Table (1).

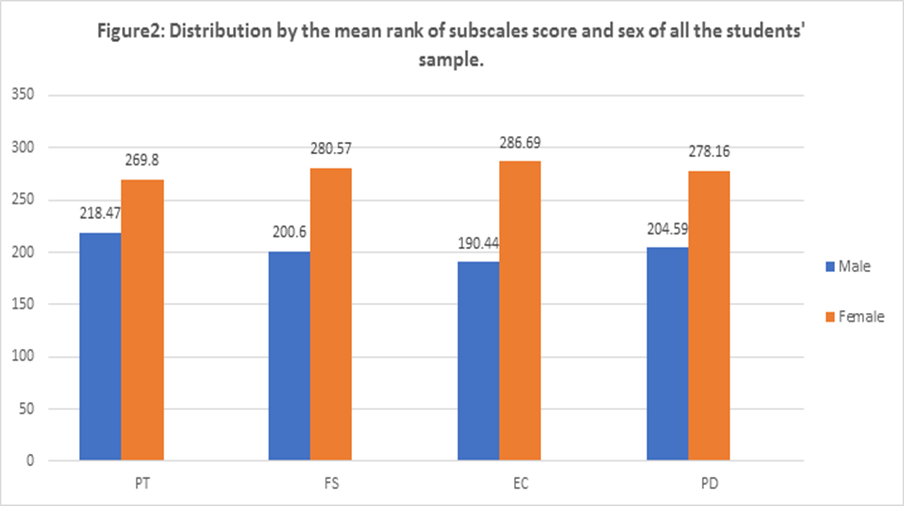
Gender and level of empathy among SQU medical students
The mean rank of scores on these sub-scales was categorized according to gender (Figure. 2 with a significant P-value (p-value<0>
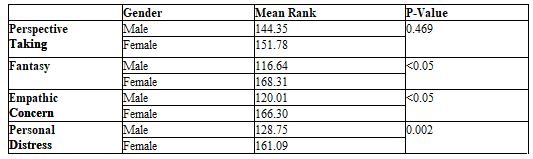
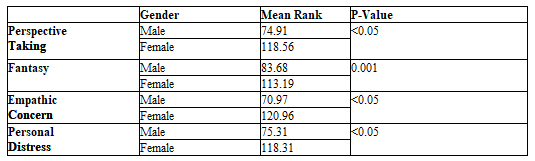
We further classified each gender according to the study phase, as shown in Tables 2 and 3. Female medical students still had higher empathy levels in all four sub-scales when we separated the data according to the study phase, with a significant p-value (P<0>p-value = 0.469).
IRI sub-scales and phase of the study:
Medical students were divided into two main groups according to their study curriculum at the College of Medicine at SQU: pre-clinical students (first through the fourth year) and clinical students (fifth through the seventh year). To compare the two groups and find the association between the phase of the study and IRI sub-scales, we used the Mann-Whitney U test. Table 4 below compares the mean rank of the four sub-scales of IRI between the two groups. There was a significant decrease (p <0>
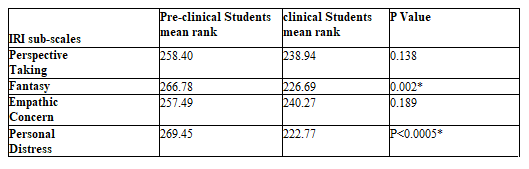
*P-value less than 0.05 is considered significant
IRI sub-scales mean and specialty of choice:
The Mann-Whitney U test was used to compare and find out the association between IRI sub-scales mean scores and the present preferable medical specialty among pre-clinical and clinical medical students.
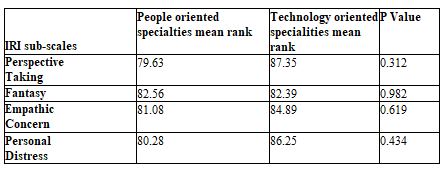
For pre-clinical students, table 5 shows the mean scores of perspectives
taking, Empathic concern and Personal distress scales to be insignificantly (p > 0.05) higher among those who preferred people-oriented specialties. On the other hand, the Fantasy means the score was insignificantly (p > 0.05) higher among those who chose technology-oriented specialties.
*P-value less than 0.05 is considered significant
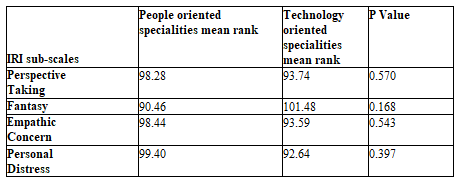
Table 6 below shows the association between the IRI and the future specialty of choice. Perspective-taking, empathic concern, and personal distress Fantasy means the score was insignificantly higher among those who preferred people-oriented specialties mean scores were insignificantly higher among those who chose technology-oriented things. The Fantasy means the score was insignificantly higher among those who preferred people-oriented specialties.
*P-value less than 0.05 is considered significant
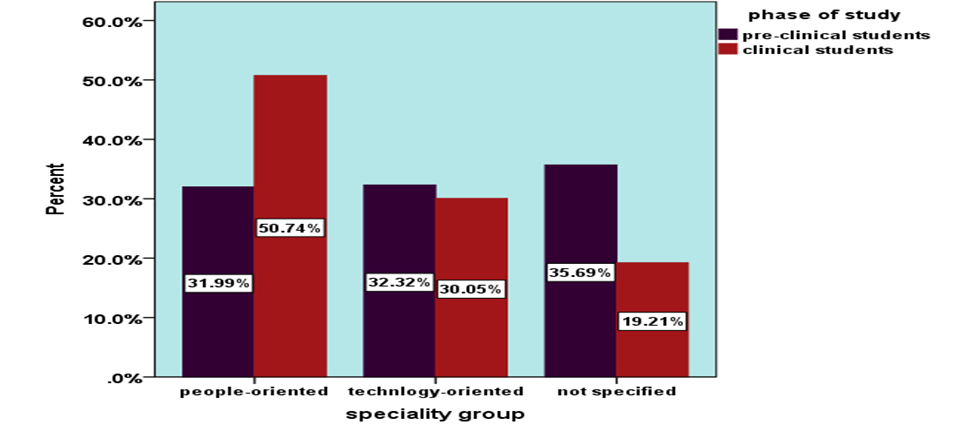
The phase of the study and preferred specialty:
The bar chart below represents the distribution by percentage of students in both phases and their preferred groups of medical specialties. Among pre-clinical medical students, 31.99Percentage of them were people-oriented specialties, and 32.32Percentage preferred technology-oriented specialties, whereas 35.69Percentage did not choose a specialty. For the clinical phase group of students, 50.74Percentage preferred people-oriented specialties, and 30.05Percentage chose technology-oriented specialties, whereas 19.21Percentage did not decide which specialty they wanted. There was a higher preference for people-oriented specialties among clinical students (1.7 times higher) than pre-clinical students. There was a slightly higher preference for technology-oriented specialties among clinical medical students. There was a higher proportion of pre-clinical students who were unsure of which specialty they prefer to join (35.69Percentage) compared to only 19.21Percentage of clinical students.
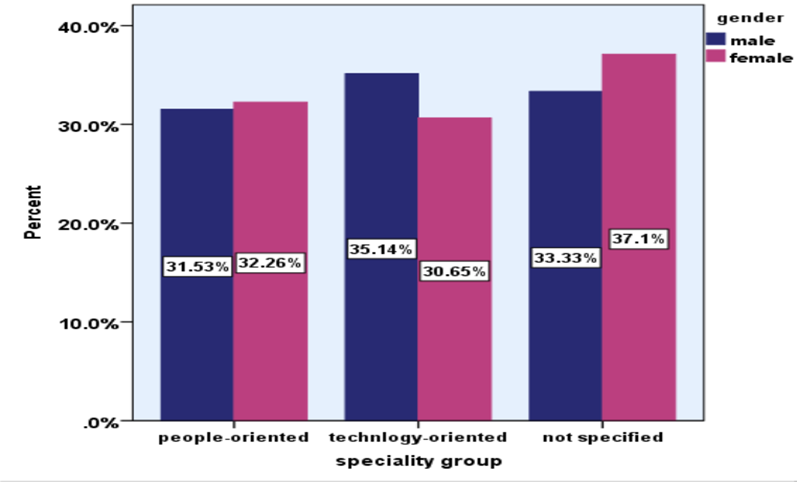
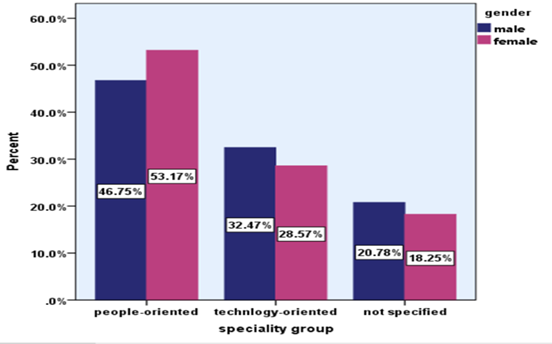
Gender and preferred specialty:
In the pre-clinical phase, as shown in graph 1, females (32.26Percentage) were more interested in people-oriented specialties than males (31.53Percentage). Males were more interested in technology-oriented specialties (35.14Percentage) than females (30.65Percentage). Out of this group, 33.33Percentage of males and 37.1Percentage of females did not decide what specialty to choose. In the clinical phase, as shown in graph 2, females' proportion was higher (53.17Percentage) for the people-oriented specialties than that of males (46.75Percentage). More males (32.47Percentage) chose this group for the technology-oriented specialties than females (28.57Percentage). There were 20.78Percentage of males and 18.25Percentage of females remained not decided.
Male and female distribution according to their present specialty preference
Discussion
This study is the first of its kind in the Sultanate of Oman. It aimed to assess the level of clinical empathy among SQU medical students and to determine the relationship between the gender and the level of clinical empathy.
After we obtained the mean and SD among SQU medical students, we compared our results with other countries that used the IRI survey in their data collection: United Kingdom (UK), New Zealand, and Ireland. SQU medical students had lower scores in EC (18.73±4.54) comparing to UK (21.18±4.03), New Zealand (20.93±4.20), and Ireland (21.15±4.02). Moreover, SQU medical students had a lower score in PT (17.75±4.04) than medical students in the UK (19.35±4.28), New Zealand (19.04±4.47), and Ireland (19.16±4.34). In PD, SQU medical students get a higher score (14.95±4.44) compared to UK (10.96±4.54), New Zealand (11.88±4.47), and Ireland (10.51±5.11), with a significant p-value in all these sub-scales (P less than0.05) [10].
Through these results, we have found that SQU medical students have lower scores in EC and PT than medical students in UK, New Zealand, and Ireland. As explained previously, PT assesses how someone can perceive the other person's point of view, while EC considers others' feelings and concerns. So, both are essential to help in communication, understanding, and dealing with the patients. On the other hand, SQU medical students got higher personal distress scores than UK, New Zealand, and Ireland. PT measures personal feelings of anxiety and its inability to deal with emergencies [10], which medical students consider undesirable characteristics. This has been said; although empathy is an essential part of being a good doctor, emotional balance is also necessary. Therefore, they should not become too emotional in emergencies.
This also can be explained based on the nature of our medical education at the university. Our medical education is more science-oriented. So, communication and empathic skills training aspects have received less attention. As a result, students focus more on theoretical knowledge, and become less interested in empathic skills, while.
Many reasons explain the differences found in empathy between medical students at SQU and other countries. For example, Social differences and living with parents until a late age makes students in our university less dependent on themselves. Thus, as a result, makes they are in a difficult position when exposed to emergencies. Moreover, patients in our society tend to refuse to talk and open up about their secrets and private lives, making it difficult for medical students to understand what they are going through.
Those skills are now considered a significant part of all UK medical schools [10]. Furthermore, a European medical education guide suggests that assessing and enhancing empathy must be considered an educational aspect, not just a desirable thing [11].
Gender and level of empathy among SQU medical students
This study reported a higher overall empathy level among female medical students at SQU. This result was similar to other studies in areas such as Kuwait and Saudi Arabia [12]. Similar results were obtained in UK, New Zealand, and Ireland, in which all used IRI in their studies. (Quince et al., 2016). Generally speaking, several factors can explain a higher empathy level of females compared to males. Firstly, neural evidence showed that the areas responsible for empathy in the limbic system are more developed in females' brains than males' brains [6]. Secondly, the influence of society and the fact that everyone, including patients, expects to find more emotional behavior while dealing with females will make females more emotional to reach the satisfaction of their patients and patient's families.
When gender was classified according to the phase of the study, it showed the same results as the general classification, with the exception of PT in which there was no significant difference between males and females in pre-clinical students. The PT assesses the other person’s point of view [10]. The reason that can explain this result is not clear, but it might be explained that pre-clinical students have not understood the concept of dealing with patients and how to react with their opinions yet. So, they answered the questions without previous exposure to a similar situation. Furthermore, the sample size might play a critical role in the difference between the two groups.
Clinical empathy and year of study:
This study found that the mean empathy score was lower among the older students' group (clinical students) compared to the pre-clinical group, with a significant decrease in the Fantasy and personal distress scales and insignificant reduction in the perspective-taking and empathic concern scales. The nature of the curriculum is different among the two student groups. Pre-clinical students are not exposed to clinical practice, nor are they used for the hospital settings, unlike clinical students, who regularly have hospital rotations and are very frequently exposed to real-life patients and are very used to the hospital atmosphere. Pre-clinical students mainly deal with clinical cases only in a theoretical manner. This difference between the two groups might explain the empathy level decrease in all IRI sub-scales. Clinical students' exposure to actual patients and their dealing with difficult situations contributed to their lower level of empathy. They undergo a lot of stress associated with night shifts, large studying materials, and many practice exams. A study showed that stress causing burnout is a significant reason to lower empathy among students [13]. Another possible outcome of the stress, along with the night shifts, is the lack of sleep. A study showed a decline in all the IRI subscales for empathy for interns who experienced lack of sleep with a significant decrease in the fantasy and personal distress subscales (P= 0.001, P=0.002, respectively) [14]. Depression associated with stress can play a role in decreasing empathy levels as well. A study showed that the presence of depressive symptoms among students had a negative correlation with the empathy levels (P less than 0.02), and it was independent of gender [13]. A study done among dental students showed a decline in empathy among students exposed to the clinical settings compared to the first-year students [15]. Our study findings were consistent with those of the Iraq study regarding higher empathy levels among pre-clinical students [16]. It was also compatible with the King Abdulaziz University study findings [12].
Clinical empathy and specialty preference:
In this study, it was observed that there was an insignificant decrease of perspective-taking, empathic concern, and personal distress scales among pre-clinical medical students for those who preferred technology-oriented specialties. The fantasy score was insignificantly increased among the technology-oriented group compared to the people-oriented. For clinical students, an insignificant increase in the perspective-taking, empathic concern, and personal distress scales was noticed among students who chose technology- oriented specialties. The fantasy score was insignificantly increased among the people-oriented group. Pre-clinical students generally showed a higher preference for technology-oriented medical specialties than clinical students (32.32Percentage versus 30.05Percentage). Clinical students' selection for people-oriented specialties was higher than pre-clinical students (50.74Percentage versus 31.99Percentage).
The results in our study opposed the findings of Iraq study in which the students' group with the higher empathy scores had a higher preferability for people- oriented specialties [16]. Another study found that higher empathy levels were associated with a preference for people- oriented medical specialties [17]. People- oriented specialties require a frequent contact with the patients, so that indeed requires a certain level of empathy and emotional intelligence, and social skills to provide the best care possible. On the other hand, technology- oriented specialties where the physician is mainly dealing with objects and devices, so they do not require a high level of empathy.
Limitations
The limitations of this study encompass the absence of a cut-off point in IRI to classify empathy levels high and low levels to know precisely where SQU medical students are located on this scale. Additionally, although Arabic countries conducted the same type of study, they used the Jefferson scale of empathy. Hence, we could not compare it with our study results statically, which might help us know more factors that can affect empathy level in the regional and cultural aspects. Moreover, other countries such as the UK, Ireland, and New Zealand didn't include the FS in their studies, so results couldn't be compared statistically to find any relationship between the level of empathy among medical students at SQU and other countries based on the FS.
Acknowledgment
None.
Conflicts of interest
None.
References
- Altena, E., Baglioni, C., Espie, C. A., Ellis, J., Gavriloff, D., et al. (2020). Dealing with sleep problems during home confinement due to the COVID‐19 outbreak: Practical recommendations from a task force of the European CBT‐I Academy. Journal of Sleep Research, 29(4).
View at Publisher | View at Google Scholar - Anand, V., Verma, L., Aggarwal, A., Nanjundappa, P., & Rai, H. (2021). COVID-19 and psychological distress: Lessons for India. PLOS ONE, 16(8), e0255683.
View at Publisher | View at Google Scholar - Arafa, A., Mohamed, A., Saleh, L., & Senosy, S. (2021). Psychological Impacts of the COVID-19 Pandemic on the Public in Egypt. Community Mental Health Journal, 57(1), 64–69.
View at Publisher | View at Google Scholar - Ayalew, M., Deribe, B., Abraham, Y., Reta, Y., Tadesse, F., et al. (2021). Prevalence and determinant factors of mental health problems among healthcare professionals during COVID-19 pandemic in southern Ethiopia: multicentre cross-sectional study. BMJ Open, 11(12), e057708.
View at Publisher | View at Google Scholar - Bergmann, M., & Wagner, M. (2021). The Impact of COVID-19 on Informal Caregiving and Care Receiving Across Europe During the First Phase of the Pandemic. Frontiers in Public Health, 9.
View at Publisher | View at Google Scholar - Buysse, D. J., Reynolds, C. F., Monk, T. H., Berman, S. R., & Kupfer, D. J. (1989). The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Research, 28(2), 193–213.
View at Publisher | View at Google Scholar - Choi, E. P. H., Hui, B. P. H., & Wan, E. Y. F. (2020). Depression and Anxiety in Hong Kong during COVID-19. International Journal of Environmental Research and Public Health, 17(10), 3740.
View at Publisher | View at Google Scholar - Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A Global Measure of Perceived Stress. Journal of Health and Social Behavior, 24(4), 385.
View at Publisher | View at Google Scholar - Cooke, J. E., Eirich, R., Racine, N., & Madigan, S. (2020). Prevalence of posttraumatic and general psychological stress during COVID-19: A rapid review and meta-analysis. Psychiatry Research, 292, 113347.
View at Publisher | View at Google Scholar - del Rio, C., Collins, L. F., & Malani, P. (2020). Long-term Health Consequences of COVID-19. JAMA, 324(17), 1723.
View at Publisher | View at Google Scholar - Deng, J., Zhou, F., Hou, W., Silver, Z., Wong, C. Y., et al. K. (2021). The prevalence of depression, anxiety, and sleep disturbances in COVID‐19 patients: a meta‐analysis. Annals of the New York Academy of Sciences, 1486(1), 90–111.
View at Publisher | View at Google Scholar - Elkayal, M. M., Shahin, M. A. H., & Hussien, R. M. (2022). Psychological distress related to the emerging COVID-19 pandemic and coping strategies among general population in Egypt. Journal of the Egyptian Public Health Association, 97(1), 3.
View at Publisher | View at Google Scholar - Gausman, J., & Langer, A. (2020). Sex and Gender Disparities in the COVID-19 Pandemic. Journal of Women’s Health, 29(4), 465–466.
View at Publisher | View at Google Scholar - GebreEyesus, F. A., Tarekegn, T. T., Amlak, B. T., Shiferaw, B. Z., Emeria, M. S., et al. (2021). Levels and predictors of anxiety, depression, and stress during COVID-19 pandemic among frontline healthcare providers in Gurage zonal public hospitals, Southwest Ethiopia, 2020: A multicenter cross-sectional study. PLOS ONE, 16(11), e0259906.
View at Publisher | View at Google Scholar - Idris, A., & Akhir, N. M. (2021). COVID-19 Pandemic: Are Caregivers of Family Members with Depression at Risk?.
View at Publisher | View at Google Scholar - Jahrami, H., BaHammam, A. S., Bragazzi, N. L., Saif, Z., Faris, M., et al. (2021). Sleep problems during the COVID-19 pandemic by population: a systematic review and meta-analysis. Journal of Clinical Sleep Medicine, 17(2), 299–313.
View at Publisher | View at Google Scholar - Khubchandani, J., Sharma, S., Webb, F. J., Wiblishauser, M. J., & Bowman, S. L. (2021). Post-lockdown depression and anxiety in the USA during the COVID-19 pandemic. Journal of Public Health, 43(2), 246–253.
View at Publisher | View at Google Scholar - Lakhan, R., Agrawal, A., & Sharma, M. (2020). Prevalence of Depression, Anxiety, and Stress during COVID-19 Pandemic. Journal of Neurosciences in Rural Practice, 11(04), 519–525.
View at Publisher | View at Google Scholar - Muldrew, D. H. L., Fee, A., & Coates, V. (2021). Impact of the COVID‐19 pandemic on family carers in the community: A scoping review. Health & Social Care in the Community.
View at Publisher | View at Google Scholar - Pérez-Cano, H. J., Moreno-Murguía, M. B., Morales-López, O., Crow-Buchanan, O., English, J. A., et al. (2020). Anxiety, depression, and stress in response to the coronavirus disease-19 pandemic. Cirugia y Cirujanos, 88(5), 562–568.
View at Publisher | View at Google Scholar - Rahimi, T., Dastyar, N., & Rafati, F. (2021). Experiences of family caregivers of patients with COVID-19. BMC Family Practice, 22(1), 137.
View at Publisher | View at Google Scholar - Rehman, U., Shahnawaz, M. G., Khan, N. H., Kharshiing, K. D., Khursheed, M., et al. (2021). Depression, Anxiety and Stress Among Indians in Times of Covid-19 Lockdown. Community Mental Health Journal, 57(1), 42–48.
View at Publisher | View at Google Scholar - Rias, Y. A., Rosyad, Y. S., Chipojola, R., Wiratama, B. S., Safitri, C. I., et al. (2020). Effects of Spirituality, Knowledge, Attitudes, and Practices toward Anxiety Regarding COVID-19 among the General Population in INDONESIA: A Cross-Sectional Study. Journal of Clinical Medicine, 9(12), 3798.
View at Publisher | View at Google Scholar - Rodríguez-Hernández, C., Medrano-Espinosa, O., & Hernández-Sánchez, A. (2021). Salud mental de los mexicanos durante la pandemia de COVID-19. Gaceta medica de Mexico, 157(3).
View at Publisher | View at Google Scholar - Salari, N., Khazaie, H., Hosseinian-Far, A., Khaledi-Paveh, B., Kazeminia, M., et al. (2020). The prevalence of stress, anxiety and depression within front-line healthcare workers caring for COVID-19 patients: a systematic review and meta-regression. Human Resources for Health, 18(1), 100.
View at Publisher | View at Google Scholar - Serafini, G., Parmigiani, B., Amerio, A., Aguglia, A., Sher, L., et al. (2020). The psychological impact of COVID-19 on the mental health in the general population. QJM: An International Journal of Medicine, 113(8), 531–537.
View at Publisher | View at Google Scholar - Sheth, K., Lorig, K., Stewart, A., Parodi, J. F., & Ritter, P. L. (2021). Effects of COVID-19 on Informal Caregivers and the Development and Validation of a Scale in English and Spanish to Measure the Impact of COVID-19 on Caregivers. Journal of Applied Gerontology, 40(3), 235–243.
View at Publisher | View at Google Scholar - Sozański, B., Ćwirlej-Sozańska, A., Wiśniowska-Szurlej, A., Jurek, K., Górniak, P., et al. (2021). Psychological responses and associated factors during the initial stage of the coronavirus disease (COVID-19) epidemic among the adult population in Poland - a cross-sectional study. BMC Public Health, 21(1), 1929.
View at Publisher | View at Google Scholar - Tee, M. L., Tee, C. A., Anlacan, J. P., Aligam, K. J. G., Reyes, P. W. C., et al. (2020). Psychological impact of COVID-19 pandemic in the Philippines. Journal of Affective Disorders, 277, 379–391.
View at Publisher | View at Google Scholar - Vizheh, M., Qorbani, M., Arzaghi, S. M., Muhidin, S., Javanmard, Z., et al. (2020). The mental health of healthcare workers in the COVID-19 pandemic: A systematic review. Journal of Diabetes & Metabolic Disorders, 19(2), 1967–1978.
View at Publisher | View at Google Scholar - Zhang, Y., Chen, Y., Wang, J., Deng, Y., Peng, D., et al. (2020). Anxiety Status and Influencing Factors of Rural Residents in Hunan During the Coronavirus Disease 2019 Epidemic: A Web-Based Cross-Sectional Survey. Frontiers in Psychiatry, 11.
View at Publisher | View at Google Scholar
