

Case Report | DOI: https://doi.org/10.31579/2835-7957/002
An Unusual Case of Endometritis After Caesarean Section
1 Department of Obstetrics and Gynecology, Faculty of Medicine, Astrakhan State Medical University, Russia.
2 Department of Obstetrics and Gynecology, Faculty of Pediatrics, Astrakhan State Medical University, Russia.
*Corresponding Author: Sergey P. Sinchikhin, Department of Obstetrics and Gynecology, Faculty of Medicine, Astrakhan State Medical University, Russia.
Citation: Sergey P. Sinchikhin, Irina V. Telegina, Roman V. Pavlov. (2022). An Unusual Case of Endometritis After Caesarean Section. Reviews and Case Reports.1(1); DOI:10.31579/2835-7957/002
Copyright: © 2022 Sergey P. Sinchikhin, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 16 September 2022 | Accepted: 28 September 2022 | Published: 06 October 2022
Keywords: reverden suture; caesarean section; endometritis
Abstract
The article describes a rare case of endometritis after delivery by Cesarean section due to ischemia and necrosis of the uterine tissue when using the Reverden suture, as well as the development of a signifi-cant local inflammation caused by the individual reaction on the suture material. Complex conservative management of endometritis with a positive outcome of organ-preserving tactics in terms of ischemic and necrotic changes in the uterus was shown.
Introduction
Over the past two decades, the total number of abdominal deliveries has increased significantly in many countries. In Eastern Europe, the Caesarean section rate varies between 24–67% [1, 2]. In our opinion, the optimal frequency of Caesarean section with a positive impact on perinatal and maternal outcomes should be the following: for the first level of obstetric care (rural obstetric facilities) – 5-10%, for the second level of obstetric care (municipal maternity hospitals) – 20-25%, for the third level of obstetric care (regional perinatal centers) – 25-35%, and up to 50% of all deliveries – in specialized obstetric research centers [3, 4].
There are several established modifications of the Caesarean section technique. Numerous studies have shown the advantages and disadvantages of different modifications. However, the research on uterine tissue repair after cesarean section depending on the method of suturing the intraoperative incision and the type of suture material requires further attention.
Patient N., 24 years old, was urgently admitted to the gynecological department of a multidisciplinary municipal hospital. Upon admission, the patient complained of purulent vaginal discharge, pain in the lower abdomen, and an increase in body temperature up to 38°C for two days. Three weeks ago, she was discharged from the municipal maternity hospital after the first emergency operative delivery by Caesarean section due to cephalopelvic disproportion during labor. There were no complications during the gestational period. The abdominal delivery was performed at 41 weeks of gestation with an intraoperative blood loss of 650 ml. Intravenous administration of a single dose of antibiotic (amoxicillin 1.2 g with clavulanic acid) was performed during the operation. The newborn with a body weight of 3360 g at delivery, with an Apgar score of 8 points in the first and fifth minute after delivery was discharged together with the mother.
The uterine incision was sutured with a single-row Reverden suture using polyglycolide as the suture material. This suture provides reliable surgical hemostasis and good tissue matching. However, some authors indicate that when the stitch width is less than 0.6 cm, tissue ischemia may occur with subsequent necrosis [4, 5, 6, 7].
Polyglycolic Acid Suture is a synthetic absorbable monofilament copolymer of glycolide and trimethylene carbonate, with high antimicrobial properties and a long resorption period (60-90 days). However, it can induce a local and (or) general inflammatory reaction [8].
According to the results of clinical, laboratory, and instrumental examinations at the discharge summary, no pathological changes were detected during the postpartum period in the maternity hospital. On the 5th day of the postoperative period, the puerperal was discharged together with the newborn.
The patient denied extragenital and gynecological diseases. There was no contact with patients infected with a new coronavirus infection over the past 14 days.
At the time of examination upon admission to the gynecological department, the patient's condition was stable. The pulse rate was 80 beats per minute, satisfactory. Blood pressure – 110/70 mm Hg. The respiratory rate is 16 per minute. Body temperature – 37 ° C. Sp O2 (saturation) – 99%.
The patient decided to refuse to breastfeed. The mammary glands were soft and painless.
The postoperative suture on the anterior abdominal wall had no signs of inflammation, healing was by primary intention. There was no pain on palpation of the anterior abdominal wall.
During the special gynecological examination in the speculum, a fragment of necrotic tissue with fibrin and suture material was identified in the vagina (Figure. 1).

Discharge from the cervical canal was purulent, with an ichorous odor. At the bimanual vaginal examination, the uterus was enlarged up to 8 weeks of pregnancy, soft consistency, limited mobility, and moderately painful. Appendages on both sides were not enlarged, painless. Moderate infiltration of the lateral fornix of the vagina was observed.
Upon admission and further monitoring of the patient in the gynecology department, a complex laboratory (Table 1) and instrumental examination was performed.
Parameter (Physiological values) | 1st day | 2nd day | 3rd day | 7th day |
Blood erythrocytes (3.8-5.1*10 12 / l) | 4.66*10 12 / l | 4.58*10 12 /l | 4.47*10 12 / l | 5.02*10 12 /l |
Hemoglobin (120-160 g/l) | 135 g/l | 134 g/l | 130 g/l | 146 g/l |
Blood leukocytes (4-9*10 9 /l) | 5.01*10 9 /l | 4.2*10 9 /l | 4.35*10 9 /l | 4.98*10 9 /l |
Platelets (180-320*10 9 /l) | 181*10 9 /l | 163*10 9 /l | 159*10 9 /l | 186*10 9 /l |
ESR (0-12 mm per hour) | 15 mm per hour | 12 mm per hour | 2 mm per hour | 10 mm per hour |
C-reactive protein mg/l (0-6 mg/l) | 25.3 mg/l | 18.4 mg/l | 9.6 mg/l | 4.0 mg/l |
Procalcitonin (0.02-0.046 ng /ml) | 0.066 ng /ml | 0.042 ng /ml | 0.02 ng /l | - |
Total protein, g/l (65-85 g/l) | 68 g/l | 62.9 g/l | 61 g/l | 65.1 g/l |
Urea (1.7-7.5 mmol/l) | 2.0 mmol/l | 1.2 mmol/l | 1.4 mmol/l | 2.1 mmol/l |
Creatinine (40-80 µmol /l) | 42 μmol /l | 49 μmol /l | 56 μmol /l | 61 μmol /l |
Total bilirubin (up to 17.5 μmol /L) | 5.0 μmol /l | 11.5 μmol /l | 6.4 μmol /l | 4.8 μmol /l |
Alanine aminotransferase (up to 31 U/l) | 20 U/l | 18 U/l | 22 U/l | 29 U/l |
Aspartate aminotransferase (up to 31 U/l) | 27 U/l | 17 U/l | 27 U/l | 30 U/l |
Blood glucose (3.9-5.8 mmol/l) | 4.9 mmol/l | 4.2 mmol/l | 5.0 mmol/l | 5.0 mmol/l |
Fibrinogen (2-4 g/l) | 4.1 g/l | 4.0g/l | 4.0 g/l | 4.0 g/l |
APTT (21-36 sec) | 27 sec | 30 sec | 25 sec | 33 sec |
PTI (80-110 %) | 103% | 98% | 110% | 104% |
Table 1: Results of laboratory examination
All parameters of the blood biochemical and coagulation analysis, as well as the urine analysis, were within normal limits. C-reactive protein and procalcitonin levels were slightly increased on admission and during the first days of treatment. Express test on SARS-CoV-2 (severe acute respiratory syndrome-related coronavirus – 2) was negative. Microscopy of vaginal smears revealed an increased number of leukocytes. According to the results of the PCR study, no sexually transmitted infections were identified.
According to the ultrasound examination of the pelvic organs, the uterus sizes corresponded to 8 weeks of pregnancy. Hyperechogenic inclusions with an acoustic shadow were diagnosed in a slightly enlarged uterine cavity and cervical canal. Liquid inclusions up to 16 mm in diameter were observed in the area of the postoperative suture (Figure. 2). The fluid level behind the uterus was 4 mm.

(Liquid inclusions in the area of the postoperative suture on the uterus)
According to the ultrasound of the abdominal cavity and retroperitoneal space, no pathological changes were detected. According to computed tomography of the abdominal cavity and pelvis (Figure. 3), the uterus was slightly enlarged in size, and a small accumulation of free fluid was observed to the right of the uterus. The clinical diagnosis of postpartum endometritis with necrosis and insufficiency of postoperative uterine sutures was defined.
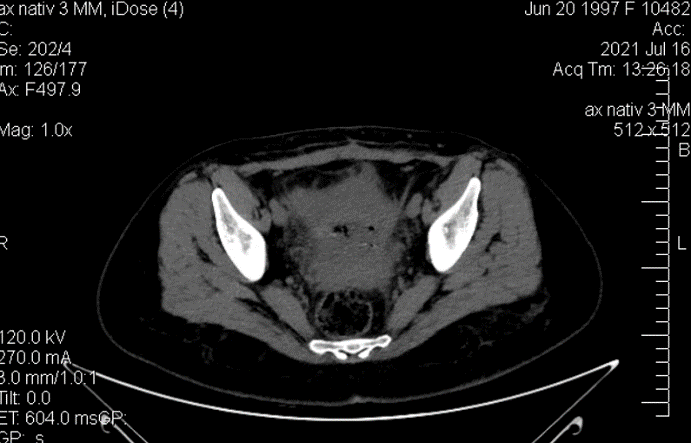
(a small accumulation of free fluid to the right of the uterus)
Taking into account the results of laboratory and ultrasound examination, the absence of a generalized inflammatory process (peritonitis) conservative management without hysteroscopy was chosen to prevent the spread of the inflammatory process and further uterine tissue damage.
The complex conservative therapy included antibacterial therapy (Meropenem 3 g per day), active drainage of the uterine cavity with antiseptics (chlorhexidine 5% water solution), and intravenous infusion therapy. Within the first three days of treatment, a decrease in pain syndrome, normalization of body temperature, a decrease in purulent discharge from the vagina, and improvement of the general status of the patient were observed. The conservative treatment continued for up to seven days.
According to the results of a microbiological study of the cervical canal discharge, the growth of Escherichia coli was detected. The histological examination of obtained material identified a necrotic tissue with fragments of suture material and multiple colonies of microorganisms.
After completion of therapy and normalization of all laboratory parameters, the patient was discharged from the hospital for further ambulatory observation and management.
Thus, complex conservative management based on a combination of systemic antibiotics of the wide spectrum with local use of antiseptics in women with the atypical clinical picture of postpartum endometritis resulted in the prevention of systemic inflammatory process and the preservation of reproductive function.
References
- Vuchenovich YuD, Olenev AS, Novikova VA, Radzinsky VE. (2019). Cesarean section: the boundaries of risks and safety. Obstetrics and Gynecology. 7(3):93-101.
View at Publisher | View at Google Scholar - Sinchikhin SP, Sarbasova AE, Stepanyan LV, Mamiev OB. (2017). Prevention of increased blood loss and coagulopathic bleeding during abdominal delivery. Gynecology. 19(1):46-50.
View at Publisher | View at Google Scholar - Abalos E, Addo V, Brocklehurst P, et al. (2016). Caesarean section surgical techniques: 3-year follow-up of the CORONIS fractional, factorial, unmasked, randomized controlled trial. Lancet. 388:62-72.
View at Publisher | View at Google Scholar - Chen Y, Han P, Wang YJ, Li YX. (2017). Risk factors for incomplete healing of the uterine incision after cesarean section. Arch Gynecol Obstet. 296:355-361.
View at Publisher | View at Google Scholar
