

Case Report | DOI: https://doi.org/10.31579/2835-7957/012
Adult Kasabach-Merritt Syndrome Associated with a Giant Liver Hemangioma; a Case Report
- R. Menoura *
- W. Tibermacine
- B. Bennia
- R. Rahmouni
- C. Balabed
- R. Achouri
- A. Delmi
Surgery department B, university hospital of Constantine Algeria.
*Corresponding Author: R. MENOURA, Surgery department B, university hospital of Constantine Algeria.
Citation: Menoura R., Tibermacine W., Bennia B., Rahmouni R., Balabed C., (2023), Adult Kasabach-Merritt Syndrome Associated with a Giant Liver Hemangioma; a Case Report. Clinical Reviews and Case Reports.2(1); DOI:10.31579/2835-7957/012
Copyright: © 2023, R. Menoura. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 31 January 2023 | Accepted: 14 February 2023 | Published: 21 February 2023
Keywords: hemangioma; giant hemangioma; kasabach-merritt syndrome; hepatectomy; ALPPS
Abstract
Hemangioma is the most common liver benign tumor, however the associated with an adult KASABACH-MERRITT syndrome is rare; to date there is no multi case report or literatures reviews are available, in the last 30 years only 17 cases have been described in the literature. we report in this work the case of a patient with a giant liver hemangioma associated to a KARABACH-MERRITT syndrome for which an ALPPS procedure have been realized.
Introduction:
The associated of Kasabach-merritt syndrome with a giant liver hemangioma cause serious coagulation disorders, which presents thrombocytopenia, hemolytic anemia, prolonged prothrombin time and hypofibrinogenemia, this association is rare in adult’s patients and most report adult’s patients are single case report [1].
Treatments are liver resection, enucleation and liver transplantation. Abnormalities in hematological and coagulative systems can return to normal after operation, A total of 17 cases were reported, with a mean age of 49.8 years (27–83 years). The size of the hemangioma was an average of 23.4cm [2, 3, 4].
Observation:
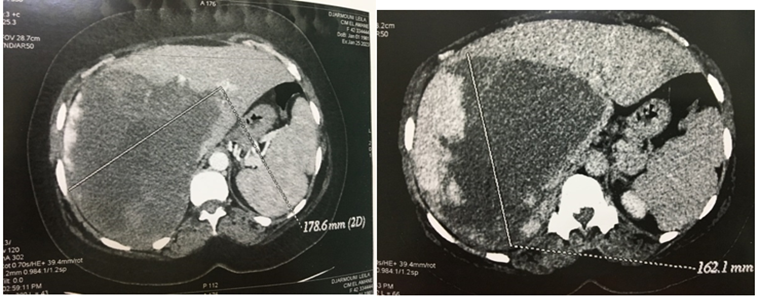
A 46 years old woman without estrogen therapy was presented to the emergency department for abdominal pain in the right hypochondrium with feeling of abdominal heaviness and generalized mucocutaneous pallor, a computed tomography scan objectified a hepatomegaly by the presence of a well limited tissue formation tacking the contrast delimiting a central hypo dense zone occupying all the right liver, mensuration’s was 29 cmX17.86cmX16.21cm (Figure 1).
She had a coagulation disorder of thrombocytopenia at 160 /mm3, anemia at 7g/L, prolonged prothrombin time at 74 percentage, and hypofibrinogenemia 69 mg/ld., D-dimers was very high at 10500 μg/L for a normal at 500 μg/L, factor V at 65 percentage, Liver enzymes were normal, tumors markers (ACE, CA19, 9, aplhafoeotprotein) were normal too and her albumin level was 30 g/l. In view of the size of the lesion and of the low hepatic volume remaining after hepatectomy an associated liver partition and portal right vein ligation for staged hepatectomy was done. Abnormalities in hematological and coagulative systems were improved after ligation and returned to normal after hepatectomy.
Discussion:
Hemangioma is the most common benign liver tumor; accounting for 73 percentage of all benign liver tumors [5], however the association with an adult Kasabach-merritt syndrome is too rare, which is more common in children and uncommon in adults, over 30 years only 17 cases was reported in literature. Giant hemangioma is all tumors with size Greater then 10 cm [6], Hemangioma are more common in middle-aged women 49.8 years, the average size was 23.4 cm; a surgical treatment was realized in 73 percentage of patients [7],
For patients with adult Kasabach-Merritt syndrome associated with giant liver hemangioma, intratumor thrombus consumed a large amount of coagulation factors, linked to an abnormal and proliferating endothelium
resulting in coagulation disorders and thrombocytopenia, which was a valid indication for surgical treatment [8, 9, 10], For patients with Kasabach-Merritt syndrome associated with liver hemangioma, the tumor is usually extremely giant, posing a significant risk during liver resection.
There was still a debate on the surgical procedures for liver hemangioma; those who are for liver resection [11, 12] and who are for enucleation.
The role of arterial embolization as a treatment for primary and secondary hepatic neoplasms is Well established [13, 14] for hepatic hemangioma and Kasabach-Merritt syndrome there are limited Data, but one report utilizing intravenous cryoprecipitate plus infusion of intra-arterial thrombin and aminocaproic acid resulted in complete stasis within the hepatic hemangioma. Unfortunately, in most cases, embolization is only temporarily effective in reducing the size of the hemangioma and improving the Bleeding diathesis [13].
Currently, the primary treatments for liver hemangioma include; liver resection, enucleation, and interventional embolism, liver transplantation has been used to treat Kasabach- Merritt syndrome associated with giant liver hemangioma, with good recovery of coagulation and platelets after transplant [15]. Enucleation is associated with a few intra-abdominal complications; it should be preferred when location and size permit [16] if not a liver resection is required.
Conclusion:
Adult Kasabach-merritt syndrome associated with a giant liver hemangioma is uncommon, Abnormalities and disorders in hematological and coagulative system return to normal after surgery. Different therapeutic options are available; enucleation, liver resection, embolization then resection and hepatic transplantation.
Conflict of Interests:
None
Funding:
None
References
- Xiaolei Liu, Zhiying Yang, Haidong Tan, Li Xu, Yongliang Sun, et al. (2017). Giant liver hemangioma with adult Kasabach-Merritt syndrome: case report and literature review, 96(31), e7688.
View at Publisher | View at Google Scholar - Tsai CC, Yen TC, Tzen KY. (1999). Pedunculated giant liver hemangioma mimicking a hypervascular gastric tumor on Tc-99m RBC SPECT. Clin Nucl Med; 24:132-133.
View at Publisher | View at Google Scholar - Ellis JV, Salzar JE, Gavant ML. (1985). Pedunculated hepatic hemangioma: an unusual cause for anteriorly displaced retroperitoneal fat. J Ultra- sound Med; 4 :623-624.
View at Publisher | View at Google Scholar - GUENOT, Claude HALLER, Raphaël ROSSO, (2004). Hémangiome caverneux pédiculé géant du foie: à propos d’un cas et revue de la littérature, Gastroenterol Clin Biol; 28 :807-810.
View at Publisher | View at Google Scholar - Toro A, Mahfouz AE, Ardiri A, et al. (2014). What is changing in indications and treatment of hepatic hemangiomas review. AnnHepatol; 13:327–339.
View at Publisher | View at Google Scholar - van Tilborg AA, Nielsen K, Scheffer HJ, et al. (2013). Bipolar radiofrequency ablation for symptomatic giant (10cm) hepatic cavernous hemangiomas: initial clinical experience. Clin Radiol ;68: e9–14.
View at Publisher | View at Google Scholar - J. Pehlivan, A.B. Beucher, K. Boudjema, C. Lacout, A. Gury, et al. (2020). Urbanski1 Élévation inexpliquée des D-dimères, penser au syndrome de Kasabach–Merritt La Revue de médecine interne 47 A90–A217.
View at Publisher | View at Google Scholar - Concerto AM, Chen CL, Chen TY, et al. (2009). Giant cavernous hemangioma of the liver with coagulopathy: adult Kasabach-Merritt syndrome. Surgery; 145:245–247.
View at Publisher | View at Google Scholar - Hochwald SN, Blumgart LH. (2000). Giant hepatic hemangioma with Kasabach-Merritt syndrome: is the appropriate treatment enucleationor liver transplantation? HPB Surg ;11 :413–419.
View at Publisher | View at Google Scholar - Longeville JH, de la Hall P, Dolan P, et al. (1997). Treatment of a giant haemangioma of the liver with Kasabach-Merritt syndrome by orthotopic liver transplant a case report. HPB Surg; 10:159–162.
View at Publisher | View at Google Scholar - Ozden I, Emre A, Alper A, et al. (2000). Long-term results of surgery for liver hemangiomas. Arch Surg; 135:978–981.
View at Publisher | View at Google Scholar - Yoon SS, Charny CK, Fong Y, et al. (2003). Diagnosis, management, and outcomes of 115 patients with hepatic hemangioma. J Am Coll Surg; 197:392–402.
View at Publisher | View at Google Scholar - Chuang, V. P. and Wallace, S. (1981). Hepatic arterial embolization in the treatment of hepatic neoplasms. Radiology, 140, 54- 58.
View at Publisher | View at Google Scholar - Steven N. Hochwald, Leslie H. Blumgar, Giant Hepatic Hemangioma with Kasabach-Merritt Syndrome" Is the Appropriate Treatment Enucleation or Liver Transplantation?
View at Publisher | View at Google Scholar - Kumashiro Y, Kasahara M, Nomoto K, et al. (2002). Living donor liver transplantation for giant hepatic hemangioma with Kasabach-Merritt syndrome with a posterior segment graft. Liver Transpl; 721–724.
View at Publisher | View at Google Scholar - Gedaly R, Pomposelli JJ, Pomfret EA, Lewis WD, Jenkins RL. (1999). Cavernous hemangioma of the liver: anatomic resection vs enucleation. Arch Surg; 134:407-411.
View at Publisher | View at Google Scholar
