

case report | DOI: https://doi.org/10.31579/2835-7957/066
Acral melanoma three years after surgery with metastasis to the breast. Case report
- Juan Mazariegos *
- Karen Pérez
- Lilian Barreda
Departamento de Patología, Hospital General San Juan de Dios, Guatemala, Guatemala.
*Corresponding Author: Juan José Mazariegos Recinos, Departamento de Patología, Hospital General San Juan de Dios, Guatemala, Guatemala.
Citation: Juan Mazariegos, Karen Pérez, Lilian Barreda. (2024), Acral melanoma three years after surgery with metastasis to the breast. Case report, Clinical Reviews and Case Reports, 3(4); DOI:10.31579/2835-7957/066
Copyright: © 2024, Juan José Mazariegos Recinos. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 February 2024 | Accepted: 20 March 2024 | Published: 08 April 2024
Keywords: metastasis; acral melanoma
Abstract
Cutaneous melanoma is the cancer with the highest mortality of skin cancers, acral melanoma is derived from epidermal melanocytes of the palm, soles, or nails, it is the most common subtype of melanoma with 2%, it occurs more in people with pigmented skin. They produce metastasis in 20% of cases and to the breast they are infrequent. We present the case of a patient with a diagnosis of acral melanoma in the right foot 6 years ago, who received treatment with remission, however three years ago she presented a recurrence with metastasis to the skin of the abdomen again with treatment and remission, currently there is a lesion in Left breast which is ulcerated and destroys the mammary stroma, the histopathological study confirms metastatic pigmented melanoma to the skin and mammary glandular tissue.
Introduction
Melanoma is a highly malignant skin tumor characterized by the excessive proliferation of atypical melanocytes. Although melanoma is frequently diagnosed in people between the sixth and seventh decades, 5.9% of detected cases occur in patients between 20 and 34 years of age. Melanoma is the most rapidly increasing cancer worldwide, with up to 20% of cases developing metastatic disease (1). There are several types of melanomas, among which acral melanoma represents 2-3% of cutaneous melanomas in the United States, this form of melanoma is located especially on the palms, soles, and periungual region. It is generally observed in older people, with an average age of 65 years, and an evolution period of 2.5 years. (2). In Guatemala, skin cancer occupies third place in frequency. In the records observed in INDERMA between January 2003 and December 2007, of 38,982 first consultations, 401 corresponded to skin cancer with a prevalence of melanoma of 0.4 per 1000 ( 3). On the other hand, in the hospital records observed in INCAN in 2004, a case prevalence of 1.5% was observed (4). In both genders, cases were reported from 30 years of age with a prevalence in the male population from 65 years of age. In general, breast metastasis from malignant melanoma referring to the acral type is rare and represents only 1.3%-2.7% of reported cases. Although breast metastases are rare, melanoma is one of the most frequently determined primary sites in patients presenting with a metastatic lump in the breast (5). In a study carried out in Guatemala, with epidemiological data by the INCAN (National Cancer Institute) was published in the year ¿?, where they concluded that the most frequent anatomical location of melanoma is the left lower limb with 71%, and it was evidenced Its relationship with Acral Lentiginous Melanoma, which occurred in 59%, presented more frequently than in an advanced metastatic stage, can spread to the breast. (6) Acranial melanoma
Case presentation
A 55-year-old female patient, originally and resident of Chiquimula, Guatemala, presented with a purplish-colored mass in the left breast with purulent discharge that had been going on for 1 year, measuring approximately 12*14 cm at the level of the upper external quadrant, with pain. to mobility intensity 7 out of 10, without fever. Medical history: acral melanoma with lesions in multiple parts of the body with chemotherapy treatment 3 years ago; acral melanoma on the skin with a diagnosis of 7 years prior with lesion on the right foot (received 25 sessions of radiotherapy, subsequently controlled foot lesion); surgical: post harvest and placement of graft in right foot post radiotherapy injury for acral melanoma 6 years ago; cholecystectomy, hysterectomy 6 years ago, appendectomy; traumatic, allergic, toxicological does not refer, gynecobstetric history with 5 pregnancies, 5 simple eutocic deliveries, no abortion, no cesarean section and date of last period 12 years ago.
Upon admission, the patient is evaluated with a physical examination: alert, active, oriented in time, space, place and person, good nutritional status, isochoric and photoreactive pupils, mobile neck without palpable lymphadenopathy, with jugular plethora present, symmetrical chest and expandable mass in the left breast. 12*24 cm, violaceous, indurated, with hematopurulent secretion, painful on palpation, lungs with adequate bilateral vesicular murmur, with predominantly basal subcrackle rales, without tactile thrill. S1 and S2 rhythmic heart synchronous with the pulse, without murmurs, flat abdomen, with gastrointestinal sounds present and normal in frequency and intensity, without signs of peritoneal irritation, without palpable masses. Extremities with normal muscle tone and strength, capillary refill of less than 3 seconds.
Complementary admission studies are performed in which leukocytes are found at 9.38 K/uL, neutrophils at 72%, hemoglobin at 13.67 gr/dl, hematocrit 47%, platelets at 231.3 K/uL, prothrombin time at 10.8 seconds, INR 1.0, thromboplastin time 21, fibrinogen 327, glucose 106 mg/dl, creatinine 0.72 mg/dl, urea nitrogen 12 mg/dl, sodium 139 mmol/L, potassium 3.8 mmol/L. Prior to admission, the patient undergoes imaging studies and biopsies on the left breast.
The patient is evaluated by the breast surgery department, indicating surgical treatment for resection of the mass and it is decided to take him to the operating room. In the operating room, a procedure is indicated for left breast cancer due to melanoma, with a Stewart-type incision, with findings of an excophytic indurated tumor +/- 10*15 cm in the left breast with axillary lymph node conglomerates of 3*3 cm, making an incision of skin and subcutaneous cellular tissue, breast tissue is dissected with a cold scalpel and electrocautery, ligation and selective hemostasis are performed, the tumor is resected until the pectoralis major muscle is exposed (figure 1).
The left axillary lymph node cluster is ligated and resected (figure B). Hemostasis is verified, fascia is closed with sucuticular stitches with 2-0 Vycril and skin with staples, two Jackson Pratt type drains are placed, with blood loss of approximately 400 cc, a procedure without complications and it is decided to send samples to the pathology department.
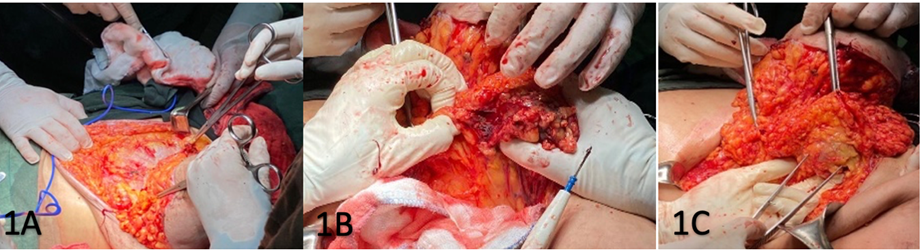
Figure 1A. Lifting of the lower flap, with dissection of subcutaneous cellular tissue to expose the pectoralis major muscle in a cephalad direction.
1B Hemostasis of external thoracic vessels to release axillary lymph node conglomerate.1C release of lymph node conglomerate and lifting of lateral flap with anterior axillary line margin.
On the fifth postoperative day, the patient tolerated a free diet, without inflammatory signs, in the breast region at the level of the surgical wound without growing hematoma, with a compressive bandage and collection of serosanguinous fluid in a Jackson Pratt drain of approximately 90 ml. Complying with antibiotic treatment with ceftriaxone, adequate evolution, it was decided to discharge by surgery, and internal medicine to program chemotherapy treatment on an outpatient basis.
The surgical piece consisted of the left breast marked with an external edge thread and two internal edge threads, which presented at the skin level two ulcerated areas measuring 2 x 1 cm and 7 x 8 cm, in the largest one a lesion of 11 x 10.5cm, black ulcerated nodular exophytic (figure 2A). The lesion cut with a depth of 10cm, black in color and firm consistency (figure 2B).
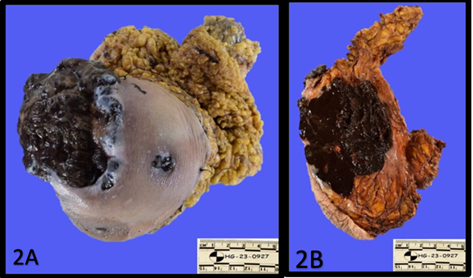
Figure 2A : Macroscopic view of the breast . Ulcerated nodular exophytic lesion. 2B: depth of injury to the breast cut.
The pathological diagnosis was pigmented melanoma metastatic to the skin and glandular breast tissue. (Figure 3 A and B).
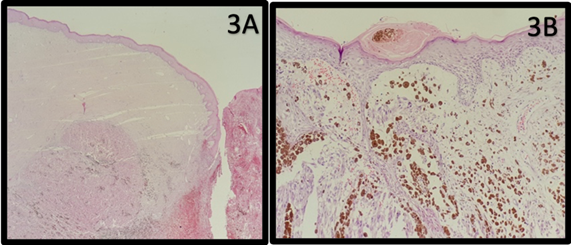
Figure 3A: skin with ulcer and neoplasia in the mammary stroma. 3B: epithelioid tumor cells with focal melanin pigment.
Discussion
.
References
- Batus M, Waheed S, Ruby C, et al. (2013). Optimal management of metastatic melanoma: current strategies and future directions. Am J Clin Dermatol; 14(3):179–194.
View at Publisher | View at Google Scholar - Portia Bradford T, Goldstein Alisa M, et. Al. (2009). Acral Lentiginous Melanoma Incidence and Survival Patterns in the United States, 1986-2005. Arch Dermatol.145(4):427-434.
View at Publisher | View at Google Scholar - National Institute of Dermatology and Skin Surgery INDERMA. http://www.indermaguatemala.com/
View at Publisher | View at Google Scholar - National Institute of Cancerology. INCAN Cancer Registry in Guatemala, Statistics Unit 2006-2010. Cancer Mortality Registry. http://regcangua.zzl.org/
View at Publisher | View at Google Scholar - Agosto-Arroyo E, Rosa M, Chau A, et al. (2017). Concurrent BRAF and PTEN mutations in melanoma of unknown origin presenting as a breast mass. SAGE Open Med Case Rep; 5:2050313X17711064.
View at Publisher | View at Google Scholar
