

Research Article | DOI: https://doi.org/10.31579/2834-8486/006
Relationship between Mental Health and Quality of Life among Health Care Workers during COVID-19 Pandemic in Vietnam
- Dung T. Phan 1,2,
- Dan T. Nguyen 3,4
- Ngoc T. Do 5
- Thuy T.T. Mai 6
- Dung T. Ha 7
- Huong T.M. Ngo 8
- Chinh D. Nguyen 9*
1 Thien An Obstetrics and Gynecology Hospital, Hanoi, Vietnam
2 Faculty of Nursing, Hanoi University of Business and Technology, Hanoi, Vietnam
3 University of Medicine and Pharmacy, Vietnam National University, Hanoi, Vietnam
4 E Hospital, Hanoi, Vietnam
5 E Hospital, Hanoi, Vietnam
6 Quang Ninh General Hospital, Quang Ninh, Vietnam
7 Bai Chay Hospital, Quang Ninh, Vietnam
8 Quang Ninh Obstetric and Pediatric Hospital, Quang Ninh, Vietnam
9 Viet Duc University Hospital, Hanoi, Vietnam.
*Corresponding Author: Nguyen Duc Chinh , Viet Duc University Hospital, Hanoi, Vietnam.
Citation: Dung T. Phan, Dan T. Nguyen, Ngoc T. Do, Thuy T.T. Mai, Dung T. Ha et al. (2022). Relationship between Mental Health and Quality of Life among Health Care Workers during COVID-19 Pandemic in Vietnam. Biomedical and Clinical Research. 1(2); DOI:10.31579/2834-8486/006
Copyright: © 2022 Chinh D. Nguyen, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 September 2022 | Accepted: 06 October 2022 | Published: 01 November 2022
Keywords: anxiety; depression, health-related quality of life; healthcare worker; nurses; patients; COVID-19; vietnam
Abstract
Background: The COVID-19 pandemic has serious consequences around the world, especially in the healthcare system. With a crucial role in the pandemic, mental health and quality of life among health care workers (HCWs) needs to be addressed.
Purposes: The study aimed to describe mental health and the health-related quality of life among HCWs and explore the relationship between mental health and quality of life among HCWs during the COVID-19 pandemic.
Methods: A cross-sectional study was conducted from 6 April to 19 April 2020 at nine hospitals in Vietnam. The questionnaire included participant's characteristics, health-related quality of life (HRQoL), Patient Health Questionnaire (PHQ), and Generalized Anxiety Disorder (GAD). De-pression and anxiety were defined as PHQ scoregreater than or equal to 10 and GAD scoregreater than or equal to 8, respectively. Descriptive, bivariate, and multiple regression analyses were used to analyze the data with a significant level at p less than 0.05.
Results: A total of 3,757 HCWs were enrolled in the study. Proportions of de-pression and anxiety were 4.5 Percentage and 3.1 Percentage, respectively. The overall mean score of HRQoL was 73.4 ± 14.9 (possible score range from 0 to 100). Protective factors of HRQoL consisted of physical activity, ability to pay for medication, gender, and social status, while its risk factors included suspected COVID-19 symptoms, smoking status. HRQoL was associated with depression (B(95 PercentageCI) = -8.15 (-10.76 to -5.55) and anxiety (B(95 PercentageCI) = -6.87 (-9.99 to -3.75)), p less than0.001.
Conclusion: There was a relationship between mental health and the health-related quality of life among HCWs. Integration of healthy lifestyles and psychological support can help improve mental health and quality of life for HCWs during the pandemic.
Introduction
One year after the World Health Organization (WHO) declared the global pandemic, Coronavirus disease (COVID-19) has rapidly spread to 223 countries and territories with over 118 million confirmed cases [1]. The COVID-19 pandemic becomes a global burden with its serious consequences, especially in the healthcare system.2-4 In Vietnam, the first phase of COVID-19 outbreak from 23 January to 5 March 2020. Although the health care system still has an imbalance situation and many hospitals face overcrowding, Vietnam had limited the pandemic by timely healthcare strategies. Thus, the entire Vietnamese health system has strong efforts during the pandemic, especially when prevention measures are prioritized [5,7]
Health care workers (HCWs), including doctors, nurses, technicians, and other support staff, play an important role in any health care system.8 While people worldwide are advised to stay at home during the pandemic, many HCWs have prolonged working under high-pressured circumstances.Besides the professionalism, their authoritative voice is crucial to promote effective COVID-19 prevention strategies. HCWs were considered as the most important resource in the COVID-19 pandemic [9-11]
During the global pandemic, HCWs have encountered many unpredictable challenges. HCWs have a high risk of COVID-19 infection in any medical setting, especially in the lack of personal protective equipment (PPE) [8,10,12]. Other occupational risks were reported, such as physical exhaustion, stigma, and discrimination. To minimize occupational risks, management strategies have been proposed, including protecting HCWs from infection, improve the capacity of HCWs, and re-arranging suitable working time [11,12].
HCWs were considered as one of the vulnerable populations in the pandemic. Besides the negative impacts on physical health, HCWs have faced mental health problems. Thus, the mental health of HCWs was considered a priority of healthcare strategies in the pandemic.13-15 Depression and anxiety were the common psychological symptoms among HCWs in the COVID-19 pandemic.17-22 To improve mental health for HCWs, psychological interventions have been promoted, mainly focusing on counseling and psychotherapies. However, most of HCWs refused to receive mental health care, but needed more rest [23,24].
In addition to mental health problems, the quality of life among HCWs was affected during the pandemic. Nevertheless, previous studies have focused on frontline HCWs and did not conclude the specific improvement measures. Research is needed to explore the relationship between mental health and quality of life among HCWs working at non-frontline areas in the COVID-19 pandemic. Therefore, the current study aimed to describe mental health, and the health-related quality of life (HRQoL); to examine factors related to depression, anxiety, and HRQoL; and to explore the relationship between mental health and HRQoL among HCWs during the COVID-19 pandemic [25-26]
Methods
Study Design, Settings, and Sampling
A cross-sectional study with a convenient sampling method was conducted at nine hospitals in Vietnam, from 6 April to 19 April 2020. Eligible participants were health care workers working at nine hospitals with ages from 20 to 60 years old and willing to take the survey. A total of 3,757 participants (61.6 Percentage of possible participants) completed the survey. The distribution of studied and possible participants at each hospital was shown in Table 1.
Name of hospitals | Possible Participants | Studied participants |
Thai Nguyen National Hospital | 1,186 | 988 |
Quang Ninh General Hospital | 922 | 683 |
Bai Chay Hospital | 819 | 476 |
General Hospital of Agricultural | 555 | 424 |
Bac Ninh Obstetrics and Pediatrics Hospital | 391 | 364 |
E Hospital | 1,125 | 335 |
Quang Ninh Obstetrics and Pediatrics Hospital | 478 | 290 |
Da Nang Oncology Hospital | 555 | 134 |
Thien An Obstetrics and Gynecology Hospital | 68 | 63 |
Total | 6,099 | 3,757 |
Table 1: Research sites and the number of participants.
Measurements
Characteristics of participants include age (years), gender (male vs. female), marital status (married, single, others), ability to pay for medication (very difficult to very easy), social status (low, middle, high), type of health care personnel (doctor, nurse, others). Participants were classified with suspected COVID-19 symptoms if they had any of the following symptoms, including common (cough, fever, dyspnea), and less common symptoms (myalgia, fatigue, headache, sore throat, sputum production, diarrhea, nausea/vomiting, chest pain, hemoptysis, confusion, and rhinorrhea).27 Comorbidity were identified by using the Charlson Comorbidity Index items and categorized into two groups (no comorbidity vs. one or more) [28] Comparing with before the pandemic, participants reported their health-related behaviors, including smoking, drinking, and physical activity, and categorized into three groups (never, stop or less, and unchanged or more). Participants were asked about their working experience (years), epidemic containment experience (yes vs. no), and accidents with biological material (yes vs. no).
The Patient Health Questionnaire (PHQ-9) has been validated and widely used in the world and in Vietnam. The PHQ-9 was used to measure depression severity including nine symptom items. Participants rated on a 4-point Likert scale from 0 (not at all) to 3 (almost every day) about the frequency of nine symptoms bothering their life during the last two weeks. The total score of PHQ ranges from 0 to 27, with the higher score indicates the higher severity of depression. PHQgreater than or equal to 10 was classified as depression disorder [29-31]
The Generalized Anxiety Disorder (GAD-7) with seven symptom items was used to assess anxiety in this study. GAD-7 is an efficient scale for evaluating anxiety severity in both research and clinical practice with good reliability and validity. Vietnamese version of GAD has been validated in the previous study [32] With a 4-point Likert scale from (not at all) to 3 (almost every day), participants were asked about the occurrence of seven symptoms during the last two weeks. The total score of GAD-7 ranges from 0 to 21, with the higher score denotes the higher severity of anxiety. Participants were classified as having anxiety disorder if they had a GAD scoregreater than or equal to 8.
Health-Related Quality of Life (HRQoL) was measured by the 36-Item Short Form Survey (SF-36), which was developed by Research and Development Corporation (RAND). The reliability and validity of this scale were investigated in previous studies. The scoring method of RAND-36 was instructed by RAND Corporation. Overall score ranges from 0 to 100, with a higher score indicates a better quality of life [33-35].
Data Collection Procedure
After obtaining institutional review board approval and permission from target hospitals, researchers provided a four-hour training session to research assistants (doctors, nurses and medical students). The training session includes data collection methods, infection prevention and control based on the World Health Organization and Vietnam Ministry of Health guidelines.8,62 All potential participants were invited to join in the study. Most of HCWs (98.3 Percentage) completed the survey by filling out the online questionnaire. The remaining participants filled out the printed questionnaires, including 8 HCWs from Quang Ninh general hospital and 56 HCWs from Thien An Obstetrics and Gynecology hospital. It took about 20 minutes for participants to complete the questionnaire. Participants could contact researchers or research assistants if they have any questions regarding to the survey. All participants completed the questionnaires without missing data due to as we used the mandatory online questions and recheck printed questionnaires by research assistants.
Ethical Consideration
This study was approved by the Institutional Review Board at the Hanoi University of Public Health in Vietnam (IRB number 133/2020/YTCC-HD3). Before collecting data at nine hospitals, ethical issues were reviewed and accepted by each hospital. Researchers ensured participants’ protection about autonomy, confidentiality, and compliance with pandemic prevention regulations.
Data Analysis
Data were analyzed by using SPSS version 20.0 (IBM Corp., Armonk, NY, USA) with a significant level at p less than 0.05. Descriptive analyses were used to describe the variables, including mean (standard deviation) and frequency (percentage). The non-normal distribution of HRQoL scores was determined by using Kolmogorov-Smirnov test. Factors related to depression and anxiety were examined by using Chi-square test for nominal or categorical independent variables and Mann-Whitney U-test for continuous independent variables. Associated factors of HRQoL were defined by using Kruskal-Wallis H-Test, Mann-Whitney U-test, and Spearman correlation for nominal, categorical and continuous independent variables, respectively.
Multiple linear regression was used to explore the relationship between mental health (depression, anxiety) and HRQoL after controlling the effect of confounding factors. Before conducting Multiple liner regression, all independent variables have been checked to ensure the correlation between each of independent variables less than 0.30. Multiple linear regression was conducted by two models. All potential confounding factors were entered in model 1, then depression and anxiety were entered in model 2.
Results
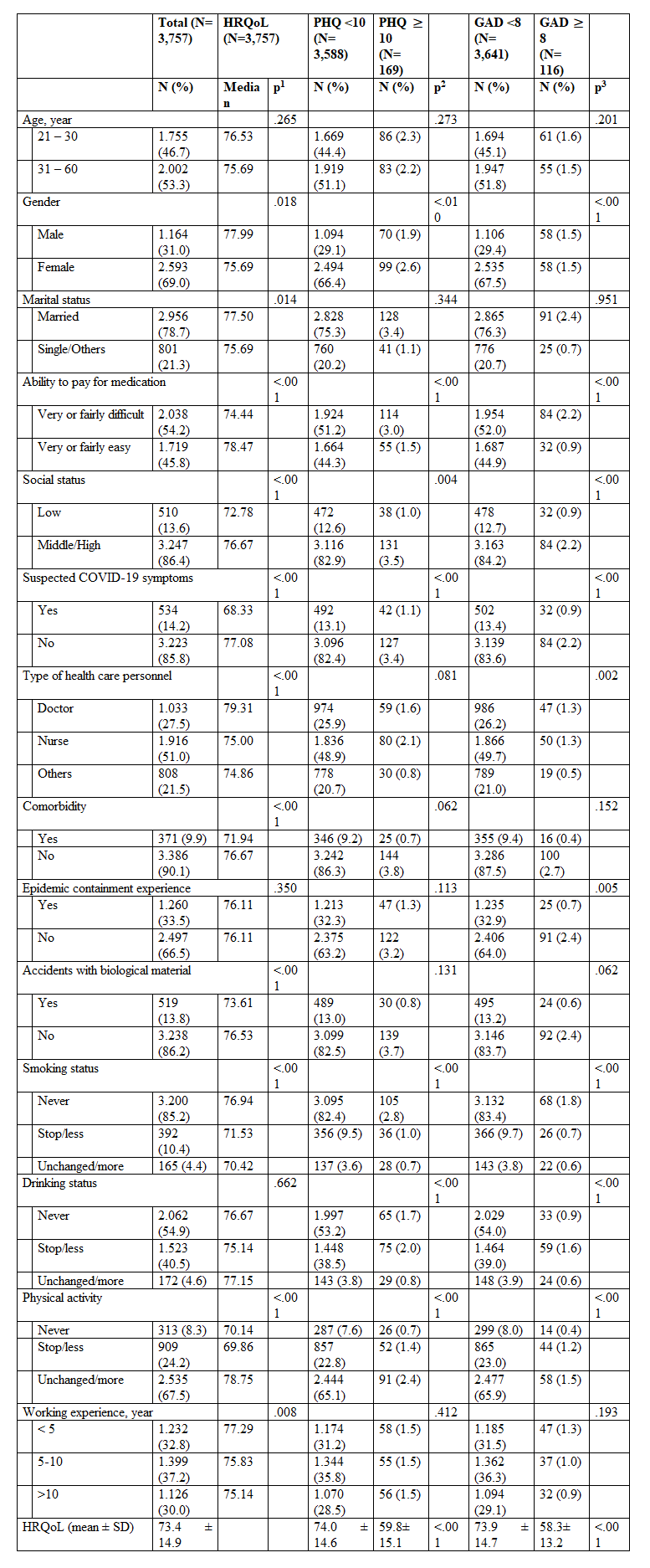
Note. HRQoL, Health-Related Quality of Life; PHQ, Patient Health Questionnaire; GAD, Generalized Anxiety Disorder; COVID-19, corona virus disease-2019; N, number; Percentage, percentage; SD, standard deviation.
Factor related to HRQoL were examined by Mann-Whitney U-test, Kruskal-Wallis H-Test, and Spearman correlation for nominal, categorical and continuous independent variables, respectively.
Factors related to depression and anxiety were examined by Chi-square test for nominal or categorical independent variables, and Mann-Whitney U-test for continuous independent variables.
p1, p2, p3, p-value of non-parametric tests for HRQoL, PHQ, GAD, respectively.
Participant’s Characteristics
In total 3.757 HCWs were enrolled in the study, the majority of participants were female (69.0 Percentage), and 53.3 Percentage of participants more than 30 years old. There was 78.7 Percentage of participants got married and 54.2 Percentage of participants had difficult ability to pay for medication. Most participants had middle or high social status (86.4 Percentage), and half of participants were nurses (51.0 Percentage). The rate of participants who had suspected COVID-19 symptoms, comorbidity, and accidents with biological material were 14.2 Percentage, 9.9 Percentage and 13.8 Percentage, respectively. Working experience of HCWs was illustrated as not much amount difference among groups less than 5 years (32.8 Percentage), 5-10 years (37.2 Percentage), and greater than 10 years (30.0 Percentage). There was 33.5 Percentage of participants had epidemic containment experience. Compare to before the COVID-19 pandemic, the proportion of unchanged or more smoking status, drinking status and physical activity were 4.4 Percentage, 4.6 Percentage, and 67.5 Percentage, respectively (Table 2).
Mental Health and Quality of Life
The overall mean score of HRQoL was 73.4 ± 14.9. The prevalence of depression and anxiety disorder among HCWs were 4.5 Percentage and 3.1 Percentage, respectively. Particularly, there were significant difference in the HRQoL score of those with depression and anxiety compare to those without depression and anxiety (p less than 0.001) (Table 2).
Factors Associated with Mental Health and Quality of Life
The HRQoL score was significantly differed in gender, marital status, ability to pay for medication, social status, suspected COVID-19 symptoms, type of health care personnel, comorbidity, accidents with biological material, smoking status, physical activity, and working experience (p less than0.05). Proportions of depression and anxiety of HCWs were varied by gender, ability to pay for medication, social status, suspected COVID-19 symptoms, smoking status, drinking status, physical activities (p less than0.05). In addition, anxiety disorder was significantly differed by type of health care personnel and epidemic containment experience (p less than0.01) (Table 2).
Relationship between Mental Health and Quality of Life
| HRQoL |
| HRQoL | ||||
| Model 1 |
| Model 2 | ||||
| B | 95 PercentageCI | p |
| B | 95 PercentageCI | p |
Gender | 1.69 | 0.65 to 2.74 | 0.001 |
| 1.75 | 0.72 to 2.78 | 0.001 |
Ability to pay for medication | 2.65 | 1.72 to 3.58 | 0.000 |
| 2.41 | 1.49 to 3.33 | 0.000 |
Social status | 1.94 | 0.58 to 3.29 | 0.005 |
| 1.57 | 0.23 to 2.90 | 0.021 |
Suspected COVID-19 symptoms | -6.44 | -7.75 to -5.14 | 0.000 |
| -5.99 | -7.28 to -4.70 | 0.000 |
Smoking | -3.32 | -4.30 to -2.34 | 0.000 |
| -2.46 | -3.44 to -1.49 | 0.000 |
Physical activity | 5.01 | 4.29 to 5.72 | 0.000 |
| 4.71 | 4.01 to 5.41 | 0.000 |
Depression |
|
|
|
| -8.15 | -10.76 to -5.55 | 0.000 |
Anxiety |
|
|
|
| -6.87 | -9.99 to -3.75 | 0.000 |
Table 3. The relationship between mental health and quality of life among HCWs using sequential multiple regression (N = 3.757)
Note. B: unstandardized coefficient; 95 Percentage CI: 95 Percentage Confidence Interval for B; p: p-value, COVID-19, corona virus disease-2019; Depression and anxiety were categorical variables.
Sequential multiple regression was used to assess the ability of depression and anxiety to predict levels of HRQoL after controlling the effect of confounding factors. After checking independent variables for the correlation between each independent variable, six confounders were retained, including gender, ability to pay for medication, social status, suspected COVID-19 symptoms, smoking status, and physical activity. In the final model, depression and anxiety were statistically significant differed in HRQoL after controlling six confounding factors. Protective factors of HRQoL including physical activity (B(95 PercentageCI) = 4.71 (4.01 to 5.41)), ability to pay for medication (B(95 PercentageCI) = 2.41 (1.49 to 3.33)), gender (B(95 PercentageCI) = 1.75 (0.72 to 2.78)), and social status (B(95 PercentageCI) = 1.57 (0.23 to 2.90)). Risk factors of HRQoL including suspected COVID-19 symptoms (B(95 PercentageCI) = -5.99 (-7.28 to -4.70)), smoking status (B(95 PercentageCI) = -2.46 (-3.44 to -1.49)). HRQoL have the relationship with depression (B(95 PercentageCI) = -8.15 (-10.76 to -5.55)) and anxiety (B(95 PercentageCI) = -6.87 (-9.99 to -3.75)) (table 3).
Discussion
In our study, female HCWs outnumbered their male counterparts (69.0 Percentage vs. 31.0 Percentage), which is consistent with the distribution of human resources for health in Vietnam.37 This was also reported in another study simultaneously conducted in Vietnam.26 Half of the HCWs in this current study were nurses (51.0 Percentage). This proportion corresponds to the one specified in a WHO’s report, stating that nurses accounted for the largest number of health workforce in Vietnam. In addition, the age distribution in the current study was similar to that in the literature [26,37].
The current study points out that HCWs had mental health problems during the COVID-19 pandemic. The findings were similar to those of other studies that reported depression and anxiety as common mental health problems among HCWs during the pandemic [17,19-22]. However, the proportions of depression and anxiety in the current study were lower than in other studies. This might be because the data collection of this current study was conducted at the beginning of the COVID-19 pandemic. Hence, longitudinal studies is recommended to explore the long-term effects of the pandemic on the mental health of HCWs.
In the last studies, HCWs with depression and anxiety reported poorer quality of life than those without these conditions. Similarly, depression and anxiety were associated with the HCWs’ reduced quality of life, as stated by prior studies [26] Thus, interventions to prevent and treat mental health problems play an important role in improving their quality of life in the pandemic. Certain previous studies indicated typical strategies to decline mental health issues, such as enhancing intensive training of infection prevention, reducing workload, expanding isolation units [38-39].
This current study also reveals that HCWs with higher levels of drinking and smoking had higher odds of depression and anxiety. These results were in concordance with those of a previous study which suggested that drinking could increase depression levels. These additional findings suggest the need for interventions to limit the effects of drinking and smoking on mental health. Like previous studies, our current study also found that women reported more depression and anxiety than men.17,19,40,41 Our study shows that HCWs with more physical activity were less likely to have mental health problems. The findings correspond to the literature in that physical activity at any level can be helpful for preventing depression. Moreover, the current study indicated that such factors as the difficulty paying for medication, low social status, and the presence of suspected COVID-19 symptoms were negatively related to the mental health of HCWs [42,43].
Using sequential multiple regression, the current study explored the relationship between the HCWs’ mental health and their HRQoL during the pandemic. More specifically, mental health problems from which HCWs suffered might contribute to lowering their HRQoL. Thus, effective interventions could benefit both their mental health and quality of life. The mental healthcare system in Vietnam is still limited; however, simple but effective coping behaviors are recommended. To cope with HCWs’ mental health problems, two most recommended behaviors were exercise and online therapeutic consultation [20]
In some current studies, physical activity was the major contributor to improving HRQoL of HCWs in the pandemic. Smoking status had a negative association with their HRQoL. The findings were also reported in certain previous studies. In addition, HCWs with suspected COVID-19 symptoms also had poorer HRQoL. Besides, male HCWs, those with better ability to pay for medication, and those with higher social status were more likely to have higher HRQoL. All of these factors should be carefully considered when psychological support is provided for HCWs as a means of promoting their quality of life [10,11,44,45].
The findings of our current study significantly contribute to further interventions for preventing HCWs’ mental health problems and improving their HRQoL, especially during the pandemic. Nevertheless, it encountered some limitations that need to be addressed. Using a cross-sectional design with a convenience sampling method might lead to selection bias, and self-report measures might affect the results to a certain extent. Therefore, longitudinal studies should be conducted to explore the holistic of HCWs’ mental health and HRQoL
Conclusion
The COVID-19 pandemic has affected HCWs’ mental health and quality of life, and depression and anxiety are associated with their quality of life. Besides psychological support, enhancing healthy lifestyles could help improve their quality of life. Our current study also demonstrated that avoiding smoking and staying physical active are behavior recommended to reducing the HCWs’ vulnerability to the COVID-19 pandemic.
References
- World Health Organization (WHO). (2020). WHO Director-General's remarks at the media briefing on 2019-nCoV on 11 February 2020. In. Geneva: WHO.
View at Publisher | View at Google Scholar - The Lancet Infectious D. (2020). Challenges of coronavirus disease 2019. The Lancet Infectious Diseases. S1473-3099(1420)30072-30074.
View at Publisher | View at Google Scholar - Gold MS, Sehayek D, Gabrielli S, Zhang X, McCusker C, et al. (2020). COVID-19 and comorbidities: a systematic review and meta-analysis. Postgraduate medicine. 1-7.
View at Publisher | View at Google Scholar - Keni R, Alexander A, Nayak PG, Mudgal J, Nandakumar K. (2020). COVID-19: Emergence, Spread, Possible Treatments, and Global Burden. Frontiers in Public Health. 8:216.
View at Publisher | View at Google Scholar - Ministry of Health. (2021). Coronavirus disease (COVID-19) outbreak in Vietnam.
View at Publisher | View at Google Scholar - Van Cuong L, Giang HTN, Linh LK, et al. (2020). The first Vietnamese case of COVID-19 acquired from China. The Lancet Infectious Diseases. 20(4):408-409.
View at Publisher | View at Google Scholar - Dinh L, Dinh P, Nguyen PDM, Nguyen DHN, Hoang T. (2020). Vietnam's response to COVID-19: prompt and proactive actions. Journal of travel medicine. 27(3).
View at Publisher | View at Google Scholar - Bielicki JA, Duval X, Gobat N, et al. (2020). Monitoring approaches for health-care workers during the COVID-19 pandemic. Lancet Infectious diseases.
View at Publisher | View at Google Scholar - Greenberg N, Docherty M, Gnanapragasam S, Wessely S. (2020). Managing mental health challenges faced by healthcare workers during covid-19 pandemic. BMJ (Clinical research ed). 368:m1211.
View at Publisher | View at Google Scholar - Department of Communications. (2020). Coronavirus disease (COVID-19) outbreak: rights,roles and responsibilities of health workers, including key considerations for occupational safety and health: Interim guidance. In: Department of Communications, ed. Geneva: World Health Organization.
View at Publisher | View at Google Scholar - Chersich MF, Gray G, Fairlie L, et al. (2020). COVID-19 in Africa: care and protection for frontline healthcare workers. Globalization and health. 16:1-6.
View at Publisher | View at Google Scholar - Greenberg N, Brooks SK, Wessely S, Tracy DK. (2020). How might the NHS protect the mental health of health-care workers after the COVID-19 crisis? Lancet Psychiatry.
View at Publisher | View at Google Scholar - Fraher EP, Pittman P, Frogner BK, et al. (2020). Ensuring and Sustaining a Pandemic Workforce. New England journal of medicine. 382(23):2181-2183.
View at Publisher | View at Google Scholar - Lima CKT, Carvalho PMM, Lima I, et al. (2020). The emotional impact of Coronavirus 2019-nCoV (new Coronavirus disease). Psychiatry Research. 287:112915.
View at Publisher | View at Google Scholar - Rana W, Mukhtar S, Mukhtar S. (2020). Mental health of medical workers in Pakistan during the pandemic COVID-19 outbreak. Asian journal of psychiatry. 51:102080.
View at Publisher | View at Google Scholar - Salazar de Pablo G, Vaquerizo-Serrano J, Catalan A, et al. (2020). Impact of coronavirus syndromes on physical and mental health of health care workers: Systematic review and meta-analysis. Journal of affective disorders. 275:48-57.
View at Publisher | View at Google Scholar - Lai J, Ma S, Wang Y, et al. (2020). Factors associated with mental health outcomes among health care workers exposed to Coronavirus disease 2019. JAMA Network Open. 3(3):e203976-e203976.
View at Publisher | View at Google Scholar - Liu CY, Yang YZ, Zhang XM, et al. (2020). The prevalence and influencing factors in anxiety in medical workers fighting COVID-19 in China: a cross-sectional survey. Epidemiology and infection. 148:e98.
View at Publisher | View at Google Scholar - Rossi R, Socci V, Pacitti F, et al. (2020). Mental Health Outcomes Among Frontline and Second-Line Health Care Workers During the Coronavirus Disease 2019 (COVID-19) Pandemic in Italy. JAMA Network Open. 3(5):e2010185.
View at Publisher | View at Google Scholar - Shechter A, Diaz F, Moise N, et al. (2020). Psychological distress, coping behaviors, and preferences for support among New York healthcare workers during the COVID-19 pandemic. General hospital psychiatry. 66:1-8.
View at Publisher | View at Google Scholar - Ma Y, Rosenheck R, He H. (2020). Psychological Stress among Health Care Professionals during the 2019 Novel Coronavirus Disease Outbreak: Cases from Online Consulting Customers. Intensive and Critical Care Nursing. 102905.
View at Publisher | View at Google Scholar - Chew NWS, Lee GKH, Tan BYQ, et al. (2020). A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain behavior and immunity.
View at Publisher | View at Google Scholar - Ko NY, Lu WH, Chen YL, et al. (2020). COVID-19-related information sources and psychological well-being: An online survey study in Taiwan. Brain, behavior, and immunity. 87:153-154.
View at Publisher | View at Google Scholar - Chen Q, Liang M, Li Y, et al. (2020). Mental health care for medical staff in China during the COVID-19 outbreak. The Lancet Psychiatry. 7:e15-e16.
View at Publisher | View at Google Scholar - Buselli R, Corsi M, Baldanzi S, et al. (2020). Professional quality of life and mental health outcomes among health care workers exposed to Sars-Cov-2 (Covid-19). Int J Environ Res Public Health. 17(17):6180.
View at Publisher | View at Google Scholar - Than HM, Nong VM, Nguyen CT, et al. (2020). Mental Health and Health-Related Quality-of-Life Outcomes Among Frontline Health Workers During the Peak of COVID-19 Outbreak in Vietnam: A Cross-Sectional Study. Risk management and healthcare policy. 13:2927.
View at Publisher | View at Google Scholar - Jiang F, Deng L, Zhang L, Cai Y, Cheung CW, et al. (2020). Review of the clinical characteristics of coronavirus disease 2019 (COVID-19). Journal of general internal medicine. 35(5):1545-1549.
View at Publisher | View at Google Scholar - Quan H, Li B, Couris CM, et al. (2011). Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. American journal of epidemiology. 173(6):676-682.
View at Publisher | View at Google Scholar - Kroenke K, Spitzer RL, Williams JB. (2001). The PHQ‐9: validity of a brief depression severity measure. J Gen Intern Med. 16(9):606-613.
View at Publisher | View at Google Scholar - Manea L, Gilbody S, McMillan D. (2015). A diagnostic meta-analysis of the Patient Health Questionnaire-9 (PHQ-9) algorithm scoring method as a screen for depression. General hospital psychiatry. 37(1):67-75.
View at Publisher | View at Google Scholar - Pham T, Bui L, Nguyen A, et al. (2019). The prevalence of depression and associated risk factors among medical students: An untold story in Vietnam. PloS one. 14(8):e0221432.
View at Publisher | View at Google Scholar - Pollack AA, Weiss B, Trung LT. (2016). Mental health, life functioning and risk factors among people exposed to frequent natural disasters and chronic poverty in Vietnam. BJPsych open. 2(3):221-232.
View at Publisher | View at Google Scholar - Hays RD, Morales LS. (2001). The RAND-36 measure of health-related quality of life. Annals of medicine. 33(5):350-357.
View at Publisher | View at Google Scholar - Vander Zee KI, Sanderman R, Heyink JW, de Haes H. (1996). Psychometric qualities of the RAND 36-Item Health Survey 1.0: a multidimensional measure of general health status. International journal of behavioral medicine. 3(2):104-122.
View at Publisher | View at Google Scholar - Jin W, Yu H. 2012). A study of the reliability and validity of SF-36 scale on evaluating health of population. Chin Health Resour. 15:265-267.
View at Publisher | View at Google Scholar - World Health Organization. (2021). Country & technical guidance - Coronavirus disease (COVID-19).
View at Publisher | View at Google Scholar - Regional Office for the Western Pacific. (2016). Human resources for health country profiles : Viet Nam. In: Manila : WHO Regional Office for the Western Pacific.
View at Publisher | View at Google Scholar - Cai H, Tu B, Ma J, et al. (2020). Psychological impact and coping strategies of frontline medical staff in Hunan between January and March 2020 during the outbreak of coronavirus disease 2019 (COVID-19) in Hubei, China. Medical science monitor: international medical journal of experimental and clinical research. 26:e924171-924171.
View at Publisher | View at Google Scholar - Mohindra R, Ravaki R, Suri V, Bhalla A, Singh SM. Issues relevant to mental health promotion in frontline health care providers managing quarantined/isolated COVID19 patients. Asian J Psychiatr. 2020;51(3):102084.
View at Publisher | View at Google Scholar - Spoorthy MS. (2020). Mental health problems faced by healthcare workers due to the COVID-19 pandemic-A review. Asian journal of psychiatry. 51:102119.
View at Publisher | View at Google Scholar - Di Tella M, Romeo A, Benfante A, Castelli L. (2020). Mental health of healthcare workers during the COVID‐19 pandemic in Italy. Journal of evaluation in clinical practice. 26(6):1583-1587.
View at Publisher | View at Google Scholar - Kvam S, Kleppe CL, Nordhus IH, Hovland A. (2016). Exercise as a treatment for depression: A meta-analysis. Journal of Affective Disorders. 202:67-86.
View at Publisher | View at Google Scholar - Mammen G, Faulkner G. (2013). Physical activity and the prevention of depression: a systematic review of prospective studies. American Journal of Preventive Medicine. 45(5):649-657.
View at Publisher | View at Google Scholar - Vogl M, Wenig CM, Leidl R, Pokhrel S. (2012). Smoking and health-related quality of life in English general population: implications for economic evaluations. BMC Public Health. 12:203.
View at Publisher | View at Google Scholar - Appleton A, James R, Larsen J. (2018). The Association between Mental Wellbeing, Levels of Harmful Drinking, and Drinking Motivations: A Cross-Sectional Study of the UK Adult Population. International journal of environmental research and public health. 15(7):1333.
View at Publisher | View at Google Scholar