

Case Report | DOI: https://doi.org/10.31579/ 2834-8419/002
L-ornithine L-aspartate and intermittent renal replacement therapy in fulminant hepatitis A: A case report
- Nourhane J. Obeid 1
- Khaled H. Soukarieh 1
- Jessy G.Fadel 2
- Rayyan M. Wazzi-Mkahal 3
- Marianne A. Alwan 3
- Jessica J. Fakhir 4
- Paul W. Rassam 1
- Najat I. Fares 3
- Mona H. Hallak 1*
1 Department of Internal Medicine, Division of Gastroenterology, Saint Georges Hospital University Medical Center, University of Balamand, Beirut, Lebanon
2 Department of Internal Medicine, Saint Georges Hospital University Medical Center, University of Balamand, Beirut, Lebanon.
3 Department of Internal Medicine, Division of Nephrology, Saint Georges Hospital University Medical Center, University of Balamand, Beirut, Lebanon
4 Department of Pharmacy, Saint Georges Hospital University Medical Center, Lebanese University , Beirut, Lebanon.
*Corresponding Author: Mona H. Hallak, Department of Internal Medicine, Division of Gastroenterology, Saint Georges Hospital University Medical Center, University of Balamand, Beirut, Lebanon.
Citation: Nourhane J. Obeid, Khaled H. Soukarieh, Jessy G.Fadel, Rayyan M. Wazzi-Mkahal, Mona H. Hallak et al. (2022). L-ornithine L-aspartate and intermittent renal replacement therapy in fulminant hepatitis A: A case report. Clinics In Radiology. 1(1); DOI:10.31579/ 2834-8419/002
Copyright: © 2022 Mona H. Hallak, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 13 September 2022 | Accepted: 19 September 2022 | Published: 30 September 2022
Keywords: children; herniotomy; experience; single surgeon; testicular atroph
Abstract
Background: Hepatitis A is a common viral infection worldwide that is transmitted via the fecal-oral route. Since the introduction of an efficient vaccine, the incidence of infection has decreased but the number of cases has risen due to widespread community outbreaks among unimmunized individuals. Classic symptoms include fever, malaise, dark urine and jaundice, and are more common in older children and adults. People are often most infectious 14 days prior to and seven days following the onset of jaundice.
Case Report: We will discuss the case of a young male patient, diagnosed with acute hepatitis A leading to fulminant hepatitis refractory to conventional therapy and the development of subsequent kidney injury. The medical treatment through the course of hospitalization was challenging and included the use of L-ornithine-L-aspartate and prolonged intermittent hemodialysis, leading to a remarkable outcome.
Conclusion: Hepatitis A is usually self-limited and vaccine-preventable; supportive care is often sufficient for treatment, and chronic infection or chronic liver disease rarely develops. However, fulminant hepatitis ,although rare, can be very challenging to manage as in the case of our patient.
Background
Hepatitis A virus (HAV) is a positive-strand RNA virus that is transmitted feco-orally through person-to-person contact [1]. Outbreaks are often linked to poor sanitation, overcrowding, or food and water contamination. According to the World Health Organization (WHO), infection rates in developed countries are low. However, high-risk groups include injection-drug users, men who have sex with men and people traveling to endemic areas and isolated communities [1]. Infection is often asymptomatic in children but adults present with jaundice, abdominal pain, hepatitis and hyperbilirubinemia. Diagnosis is through the detection of immunoglobulin M antibodies against HAV. The clinical spectrum of hepatitis A virus infection ranges from asymptomatic infection to fulminant hepatitis. Clinical manifestations depend on the age of the host: less than 30 Percentage of infected young children are symptomatic, while about 80 Percentage of infected adults manifest severe hepatitis with remarkably elevated serum aminotransferases. Fulminant hepatitis is rare, with a reported incidence of 0.015 to 0.5 Percentage [2] . Atypical manifestations include: relapsing hepatitis, prolonged cholestasis and complicated cases with acute kidney injury [2]. Extrahepatic manifestations include autoimmune hemolytic anemia, aplastic anemia, pure red cell aplasia, pleural or pericardial effusion, acute reactive arthritis, acute pancreatitis, acalculous cholecystitis, mononeuritis and Guillain-Barré syndrome [2]. Fundamental management of hepatitis A is active vaccination, supportive care and liver transplantation for fulminant hepatitis A, which awaits further studies on prognostic predictors and some therapeutic measures [3]. Our case highlights the importance of intermittent renal replacement therapy in the management of refractory fulminant hepatitis A and the hepatic role of L-ornithine-L-aspartate.
Case presentation
We herein report a case of a 38 year-old man, with a history of dyslipidemia on rosuvastatin and ezetimibe, who presented for jaundice of 1 day duration, associated with nausea and decreased PO intake since 1 week. Before the presentation, he had 2 febrile episodes for which he took only 2 tablets of paracetamol. Three weeks before presentation, the patient disclosed a previous illness encounter with a coworker who had documented hepatitis A.
Otherwise, he is a nonsmoker, a non-alcohol consumer and vaccinated against COVID-19 (2 doses, the last one was 5 months prior to presentation). He had no past surgical history, no known allergies, no drug or substance abuse, and reported a monogamous relationship and protected sexual intercourse with his girlfriend.
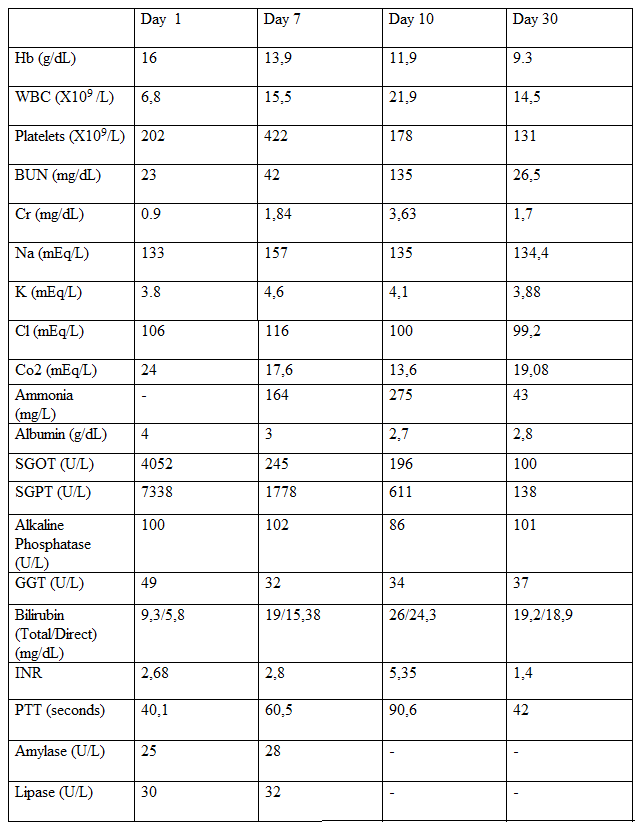
On presentation, he was hemodynamically stable and afebrile. On physical exam, he was conscious, cooperative and oriented to place, person and time. He had right upper quadrant tenderness and icteric sclera otherwise nothing was significant. His initial and follow-up laboratory values are summarized (Table 1). Covid-19 PCR was negative. Viral, bacterial and parasitic serologies ( CMV, EBV, HCV-Ab, HBs Ag, HSV, HIV, syphilis, brucella , toxoplasma ) were all negative, except for HAV IgM : 2,57 (positive) and total HAV : 0.011(index positive). AMA (anti-mitochondrial antibody) was negative, and ANA (anti-nuclear antibody) was borderline positive at a titer of 1/100. Ultrasound (U/S) abdomen and pelvis on admission showed only hepatomegaly.
The clinical decision was taken to admit the patient to the ICU for close monitoring and start him on symptomatic treatment. Serial PT and PTT were ordered every 6 hours and home medications were stopped. On day 3 of presentation, he started deteriorating. He developed grade II hepatic encephalopathy, for which he was started on lactulose 30 cc thrice per day (tid), targeting 2-4 bowel movements per day and rifaximin 200 mg 2 tablets tid with no improvement. A brain computed tomography (CT) scan was done showing mild cerebral edema but no midline shift. Based upon our expert hepatologist recommendation, the patient was started on methylprednisolone 500 mg daily, IV pulse therapy for a total of 3 days for a possible concomitant autoimmune hepatitis, and ursodeoxycholic acid (UDCA) 250 mg PO tid for pruritis.
On day 7, he got intubated for worsening encephalopathy (GCS: 7). L-ornithine, L-aspartate was added in NG tube 1 sachet tid. The patient also developed progressive acute renal failure refractory to conventional treatment as IV hydration, for which he was started on daily prolonged sessions of intermittent hemodialysis, 6 hours each, as a bridge to continuous renal replacement therapy (CRRT) for worsening kidney function and hyperammonemia . The repeated level of ANA at that time turned out to be normal.
Despite all measures, the neurological state was not improving, hence a brain MRI was requested on day 7 and showed abnormal signals in the cortex and basal ganglia including the thalamus, compatible with mild cerebral edema with no increase in intracranial pressure (ICP) and this could be reversible (metabolic in etiology). EEG done on day 10, showed diffuse slowing compatible with metabolic origin. All brainstem reflexes were preserved with response only to painful stimuli.
On day 8, the patient became febrile. All infectious workup was negative , including urine analysis ,urine culture and blood cultures, except for infiltrates on chest X-ray with no documented increase in oxygen requirement on the ventilator. He was started by an ID specialist on piperacillin/tazobactam 4,5 g IV q 6h for hospital-acquired pneumonia.
At this stage and due to the worsening of the patient’s clinical status, the hepatologist decided to start him on N-acetylcysteine (NAC) 2 sachets twice per day for its possible role in hepatic improvement even in non-acetaminophen induced hepatitis.
During his ICU stay (day 11), the patient developed 1 episode of coffee ground emesis for which he was started on IV continuous proton-pump inhibitors (PPI) and underwent urgent gastroscopy that showed erosive antral gastritis (which bled secondary to high INR level, see Table 1). He subsequently received several fresh frozen plasma (FFP) units. The emesis, then, ceased.
During the treatment course, our patient also developed watery diarrhea secondary to Clostridium difficile colitis that was treated with 10 days of oral vancomycin 125 mg q 6h after finishing piperacillin/tazobactam course.
After taking the family consent, the patient was planned to be transferred to a CRRT specialized center, as a bridge to liver transplantation. He was off sedation since the EEG date. The liver matched donor was chosen and our expert hepatologist and liver transplant specialist along with the general surgeon were on board.
Meanwhile, the nephrologist completed a total of 5 sessions of prolonged intermittent hemodialysis of 6-8 hours each session, after which the patient showed a remarkable improvement in his ammonia level, a secondary improvement of his neurological state and a subsequent improvement in his kidney function. Hence, the patient was successfully extubated on day 17 and was able to communicate with the medical team and his family. Accordingly, his laboratory values were gradually improving including liver transaminases and liver function tests (Table 1). Hence, the decision was taken to abate the liver transplantation and the transfer to a CRRT facility.
After receiving 13 days of nutritional, psychological support and physiotherapy (i.e day 30 of hospitalization), the patient was successfully discharged home on ursodeoxycholic acid and lactulose with marked improvement of his laboratory values (table 1) and was scheduled for short-interval clinic visits with follow up laboratory test.
Discussion
Acute liver failure (ALF) is defined as an acute liver insult with catastrophic consequences and no pre-existing liver disease. Its two main cardinal features are: encephalopathy and coagulopathy [4]. ALF is rare with an incidence of less than 1 Percentage. Main etiologies are drug-induced ,viral, immunologic and other causes.
The risk of ALF in acute hepatitis A is less than 1 Percentage. The majority of HAV-related ALF has a spontaneous resolution rate (~70 Percentage) and the remaining 30 Percentage require an urgent liver transplant or result in death. Cerebral edema is one of the feared complications of ALF and one of the leading causes of death.
Indications of prognosis include a creatinine level greater than 2 mg/dL, an ALT greater than 2,600 U/L, and need for intubation. These are associated with poor prognosis, in addition to other indicators such as nonalcoholic fatty liver disease and alcoholic steatohepatitis; so such patients are more likely to develop acute on chronic liver failure from HAV [5].
In our case, the patient was empirically monitored in ICU for fear of future complications. On his third day of admission, the patient had neurologic deterioration but this was not attributed to the cerebral edema as it was very mild according to the CT scan and it did not accompany a midline shift or other signs of high intracranial pressure. His brainstem reflexes were also normal. Therefore, the neurological deterioration was attributed to encephalopathy (grade II) secondary to the underlying metabolic changes from ALF and proven by the slow waves on EEG.
He was started on lactulose and rifaximin for hepatic encephalopathy, UDCA for pruritis and methylprednisolone for possible underlying autoimmune hepatitis although its clinical suspicion was very low, as plasma concentration of gamma globulins and repeated level of ANA was normal and the patient did not respond well to steroid.
However, his encephalopathy worsened and the patient became non responsive with a GCS of 7 for which he got intubated and ventilated for airway protection.
At this point, L-ornithine L-aspartate (LOLA) one sachet three times daily was started for hepatic encephalopathy refractory to conventional therapy, as the patient was still deteriorating despite appropriate treatment and supportive care as mentioned above with rising ammonia level. At this stage, he was referred for an urgent liver transplant.
L-Ornithine L-Aspartate (LOLA) is a combination of two natural amino acids, ornithine and aspartate. It can be administered orally or parenterally with major effect on the reduction of the grade of hepatic encephalopathy (HE) in clinical trials. They also had encouraging effects on psychomotor function in cirrhotic patients with minimal hepatic encephalopathy (MHE) and chronic grade I HE [6].
Several randomized controlled clinical trials (RCT) have revealed that the use of LOLA increases the removal of ammonia by residual hepatocytes and skeletal muscle of patients with cirrhosis.
Direct hepatoprotective effects of LOLA were also demonstrated in RCT, where reduction of the plasma concentrations of liver enzymes was seen, as well as improvement of liver function and amelioration of symptoms of HE in patients with cirrhosis [7,8].
Several mechanisms appear to be responsible for the protective actions of LOLA and are related to this agent’s components: L-ornithine and L-aspartate, as well as their metabolites: glutamate, glutamine, and glutathione [7].
Mechanisms of actions of LOLA
The detoxification of ammonia by the liver is based on two metabolic pathways: the synthesis of urea and the synthesis of glutamine [7,9].
LOLA acts by delivering important substrates for both pathways, and it has been shown to rise plasma levels of glutamate and glutamine when administered to cirrhotic patients.
L-aspartate is metabolized to alanine and oxaloacetate in the intestinal mucosal cells. An increase of alanine in plasma is effective in reducing increased plasma liver enzymes [7].
L-ornithine is an important activator of the urea cycle that will lead to the elimination of ammonia, especially in cases where the activities of the urea cycle enzyme are compromised [7,9].
It also increases the synthesis of glutamine in the liver and the skeletal muscle.
The increase in glutamine synthesis leads to the elimination of excess ammonia and may also be involved in the direct hepatoprotective effects of LOLA.
Glutamine has also been shown to have antioxidant properties that help in the protection of the liver. These outcomes show that LOLA manifests hepatoprotective activities by removal of ammonia and improvement of anti-oxidative capacity [6].
Another pathway of hepatoprotective actions of LOLA consists of the production of nitric oxide (NO) from L-arginine. This has been shown to result in improved hepatic microcirculation [6,7].
Circulating L-arginine is produced from L-ornithine as shown in studies of patients with HE or cirrhosis who were treated with LOLA [7].
There is a limited role for liver biopsy in ALF. However, liver biopsy is strongly indicated in cases of suspicion of malignant infiltration and cases of alcoholic hepatitis ,especially when considering a liver transplant. However, our patient was not stable enough to undergo a liver biopsy and was assigned for an urgent liver transplant. Meanwhile patient was maintained on LOLA in addition to lactulose and rifaximin. NAC was added for its predicted beneficial effect and role in non acetaminophen-induced ALF (NAI-ALF).
N-Acetylcysteine (NAC) is known to be the precursor of glutathione, a very important detoxifying agent. NAC is a potent antioxidant that helps in eliminating free oxygen radicals and replenishing cytoplasmic and mitochondrial glutathione stores [10]. NAC also enhances non-toxic sulfate conjugation by acting as a source of sulfate, thus averting hepatic impairment [11]. NAC has also been proven to have vasodilatory and inotropic effects which help ameliorate the oxygenation and perfusion of vital organs during shock states [11]. It is as an antidote to acetaminophen. But the guidelines of the American Association for the Study of Liver Diseases (AASLD) published in 2011 suggested that it may also be of importance in non-acetaminophen induced acute liver failure (NAI-ALF) [11].
A retrospective study conducted on patients with NAI-ALF, showed that patients who received NAC had an increased survival rate with their native liver as compared to patients who were not treated with NAC.
Despite all these therapeutic measures, the patient only showed mild improvement in encephalopathy and his renal function worsened. Therefore, the decision was made to start intermittent hemodialysis as our dialysis center does not provide continuous renal replacement therapy, for two main purposes: removal of ammonia through hemofiltration and improvement of renal function.
More than 80 Percentage of patients with fulminant hepatitis develop acute renal failure (ARF), which negatively influences the overall prognosis [12]. The pathophysiology of the ARF in hepatitis is not well known and different mechanisms are suggested [12]. First, volume depletion related to nausea, vomiting, and diarrhea leads to stimulation of the renin-angiotensin system and prerenal acute kidney injury. Second, immune complex-mediated nephritis where in the case of hepatitis A, may lead to different types of glomerular disorders, including membranous nephropathy, mesangial proliferative, and membranoproliferative glomerulonephritis. Third, endotoxemia related to hepatitis will lead to systemic hypotension, renal vasoconstriction, the release of cytokines and the activation of neutrophils, which will contribute to renal injury [12]. ARF is considered a cause of hyperammonemia if it occurs early with acute liver failure decreasing the ammonia excretion by 20 Percentage. Ammonia is a major regulator of acid-base homeostasis [13] and extracellular pH and plasma potassium concentration play an important role in the regulation of ammonia synthesis and transport [13]. Hypokalemia can precipitate encephalopathy by stimulating ammonia-genesis in the tubule [14] and bicarbonate-containing fluids induce cerebral vasodilation, facilitate ammonia entry in the brain and so lead to intracranial hypertension [15].
Ammonia is a 17 g/mol non-protein-bound element with a diffusive clearance similar to urea, both continuous and intermittent modalities of renal replacement therapy (RRT) are efficient to remove it from the plasma but with different rates [13,15]. The timing to start dialysis in adults with acute liver failure, hyperammonemia and cerebral edema is still unknown [13,15] . It has been suggested to consider it when the ammonia level is three times more than the upper limit of normal or when patients are severely encephalopathic, even before the advancement of AKI [13] . Continuous RRT (CRRT) used alone or with intermittent hemodialysis is considered the method of choice because it provides uninterrupted clearance for ammonia reducing post-hemodialysis rebound caused by a deferred ammonia shift from extravascular compartments [13,15] . It allows a gradual reduction in serum osmolality and less shift of water across the blood-brain barrier to prevent the worsening of cerebral edema in patients with high intracranial pressure. It also allows temperature control and slow correction of metabolic abnormalities such as hyponatremia [15] . Despite the recommended use of the CRRT, our patient has been treated with daily long sessions of intermittent dialysis with good outcomes. So, in the absence of CRRT availability, intermittent hemodialysis might still be a good option.
Conclusion
HAV continues to be a global health issue, with the highest rates in lower-income countries. Fulminant hepatitis is rare, yet the most feared complication due to the difficulty in management and the overall poor prognosis. Treatment of hepatic encephalopathy focuses on the reduction of ammonia produced in the colon. In this context, LOLA promotes ammonia clearance and increases production of glutamine, making it an excellent therapeutic alternative and could have contributed to the patient improvement along with dialysis. The use of CRRT to reduce ammonia levels in the treatment of cerebral edema has been reported in the literature, yet, in our case, the use of intermittent hemodialysis was effective despite established guidelines about the importance of CRRT in this situation. Thus, our case proves the importance of renal replacement therapy in fulminant hepatitis A with ARF refractory to standard treatment and also proves that intermittent hemodialysis can possibly be an efficient alternative, in centers who lack the CRRT. However, more studies need to be published in the future.
Financial support
None
Conflict of interest
None
Patient Consent: The patient’s written consent for the publication of this case was taken.
Acknowledgement
Dr.Bilal Hoteit, contributed to the medical file review of the patient for matching donor liver and general support.
References
- Takihara H, Cosentino MJ, Sakatoku J, Cockett AT. (1987). Significance of testicular size measurement in andrology: 11. Correlation of testicular size with testicular function. J Urol. 137(3): 416-417.
View at Publisher | View at Google Scholar - Bahk JY, Jung JH, Jin LM, Min SK. (2010). Cut-off value of testes volume in young adults and correlation among testes volume, body mass index, hormonal level, and seminal profiles. Urology. 75(6): 1318-1318
View at Publisher | View at Google Scholar - Mittal PK, Little A, Harri PA, Miller FH, Alexander LF, et al. (2017). Role of imaging in the evaluation of male infertility. Radiographics. 37(3): 837-854.
View at Publisher | View at Google Scholar - Abdelhalim A, Chamberlin JD, Young I, Fahim M, Chuang KW, et al. (2019). Testicular volume changes in laparoscopic staged Fowler-Stephen’s orchidopexy: Studying the impact of testicular vessel division. Urology. 127: 1118-1123.
View at Publisher | View at Google Scholar - Yang DM, Choi H, Kim HC, Kim SW, Moon SK, et al. (2021). Small testis: clinical characteristics and ultrasonographic findings. 40(3): 455-463
View at Publisher | View at Google Scholar - Reid I, Devlin HB. (1994). Testicular atrophy as a consequence of inguinal hernia repair. BJS. 81(1): 91-93.
View at Publisher | View at Google Scholar - Bokar NB, Kashyap NK, Mohanty D. (2015). Congenital hernias and hydrocele: Importance of age. Afr J Paediatr Surg. 12: 158.
View at Publisher | View at Google Scholar - Lee JW, Lee TY, Choi HY. (2007). Change of testicular volume after mumps orchitis. Korean J Urol. 48(5): 542-547.
View at Publisher | View at Google Scholar - Lian BS, Cheong YL, Low Y, Nah SA. (2015). Testicular atrophy: A complication of non-mumps orchitis after scrotal exploration for presumed testicular torsion. Proceedings of Singapore Healthcare. 25(3): 1-3.
View at Publisher | View at Google Scholar - Charny CW. Meranze DR. (1948). Pathology of mumps orchitis. J Urol. 60(1): 140-146.
View at Publisher | View at Google Scholar - Brainwood M, Beirne G, Fenech M. (2020). Persistence of the processus vaginalis and its related disorders. Australas J Ultrasound Med. 23(1): 22-29.
View at Publisher | View at Google Scholar - Helal AA, Daboos M, Othman A, Abdelhafez M. (2020). Single-incision percutaneous closure of pediatric inguinal hernia: A New Modification for intracorporeal suture Knotting. Minim Invasive Surg. 5610513.
View at Publisher | View at Google Scholar - Grech G, Shoukry M. (2022). Laparoscopic inguinal hernia repair in children: Article review and the preliminary Maltese experience. J Pediatr Surg. 57(6): 1162-1169.
View at Publisher | View at Google Scholar